
BLOOD PRESSURE VARIABILITY AND ARTERIAL STIFFNESS
- DOI
- 10.1016/j.artres.2011.10.001How to use a DOI?
- Keywords
- Arterial stiffness; Blood pressure variability; Wave reflections
- Abstract
Blood pressure variability (BPV) is defined by the standard deviation of a given sample of population of normotensive or hypertensive subjects. Recent studies have suggested that this parameter might constitute a cardiovascular risk factor. Reduction of blood pressure variability could be an important purpose of anti-hypertensive treatment, as suggested from experimental studies. In a double-blind controlled investigation, the thiazide compound indapamide was compared to placebo, to the angiotensin blocker candesartan and to the calcium-entry blocker amlodipine for 12 weeks treatment. The 3 drugs reduced significantly and identically blood pressure. Only indapamide and amlodipine reduced significantly BPV. This study was the first to demonstrate the interest of BPV in the setting of a double-blind, placebo controlled, trial.
- Copyright
- © 2011 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
For many decades, the main goal of antihypertensive treatment was to lower blood pressure (BP) to a defined level. For instance, if blood pressure is measured each 30 min during 24 h, the mean value of the 48 measurements may be considered as the mean BP determinations of this day. Such measurements may be performed before and after a given treatment period. The difference between the two BP measurements represents the antihypertensive effect, an oversimplified evaluation of the risk reduction under treatment. Recently, several investigators have shown that blood pressure variability (BPV) is another critical factor to consider and emphasize in the treatment of hypertension. BPV is a parameter different from mean BP. If it is supposed that, during the 24 h, the BP distribution is Gaussian, then the standard deviation of this distribution may be considered an index of BPV. Mancia et al.1 were the first to report a close association of BPV, assessed from 24-h ambulatory BP monitoring (ABPM), with target-organ damage of hypertensive patients. More recently, Rothwell2–4 showed that BP variability was an independent and strong predictor of cardiovascular events, such as stroke and coronary heart disease. In this report, our goal is, from experimental and clinical studies, to show the interest of BPV in the management of treated hypertensive subjects.
Experimental studies
In experimental animals, only two models of normotensive rats have been described to define increased BPV: baro-receptor denervation and chemical sympathectomy by guanethidine.5,6 Both procedures, in the absence of hypertension or diabetes mellitus, are associated with the same increase of BP standard deviation, but, at the same time, are characterized by different histopathological aspects: elastin alterations in chemical sympathectomy and collagen excess in baro-receptor denervation. However, both cases are associated with the same significant increase of arterial stiffness, independent of mean BP level. Taken together, all these particularities indicate the presence of associated modifications of vascular smooth muscle (VSM) cells and extra cellular matrix (ECM) which are highly involved in the mechanisms of the integrin pathways. For instance, connections between fibronectine (ECM) and integrin alpha 5- beta 1 (VSM) in the presence of pulsatile stress are able to determine a significant increase of arterial stiffness. Increased arterial stiffness may be in turn reversed by angiotensin blockade, so modifying BPV.7
Clinical studies
Recent clinical research by our group, published in July 2011 in Hypertension,8 aimed to investigate the effect of different antihypertensive agents on BP variability and the underlying mechanism. Until now, this unique effect was never shown in the setting of a randomized, double-blind, placebo-controlled study.
We analyzed the ambulatory BP monitoring data of 577 patients before and after 3-month antihypertensive treatment, in the Natrilix SR Versus Candesartan and Amlodipine in the Reduction of Systolic Blood Pressure in Hypertensive Patients (X-CELLENT) Study.9 This is a multicenter, multinational, randomized, double-blind, placebo-controlled study with 4 parallel treatment arms: placebo, indapamide sustained release (SR), amlodipine, and candesartan. Drugs were respectively a diuretic, a calcium-entry blocker and an angiotensin blocker.
Three major findings were reported. Firstly, we found that the 3 anti-hypertensive drugs had a similar BP-lowering effect (P < 0.001 for all) [Fig. 1a] but amlodipine (P < 0.05) and indapamide SR (P < 0.05) were the only agents associated with a significantly decreased 24-h systolic BP variability after 3-month treatment [Fig. 1b]. Candesartan did not reduce BP variability.8,10
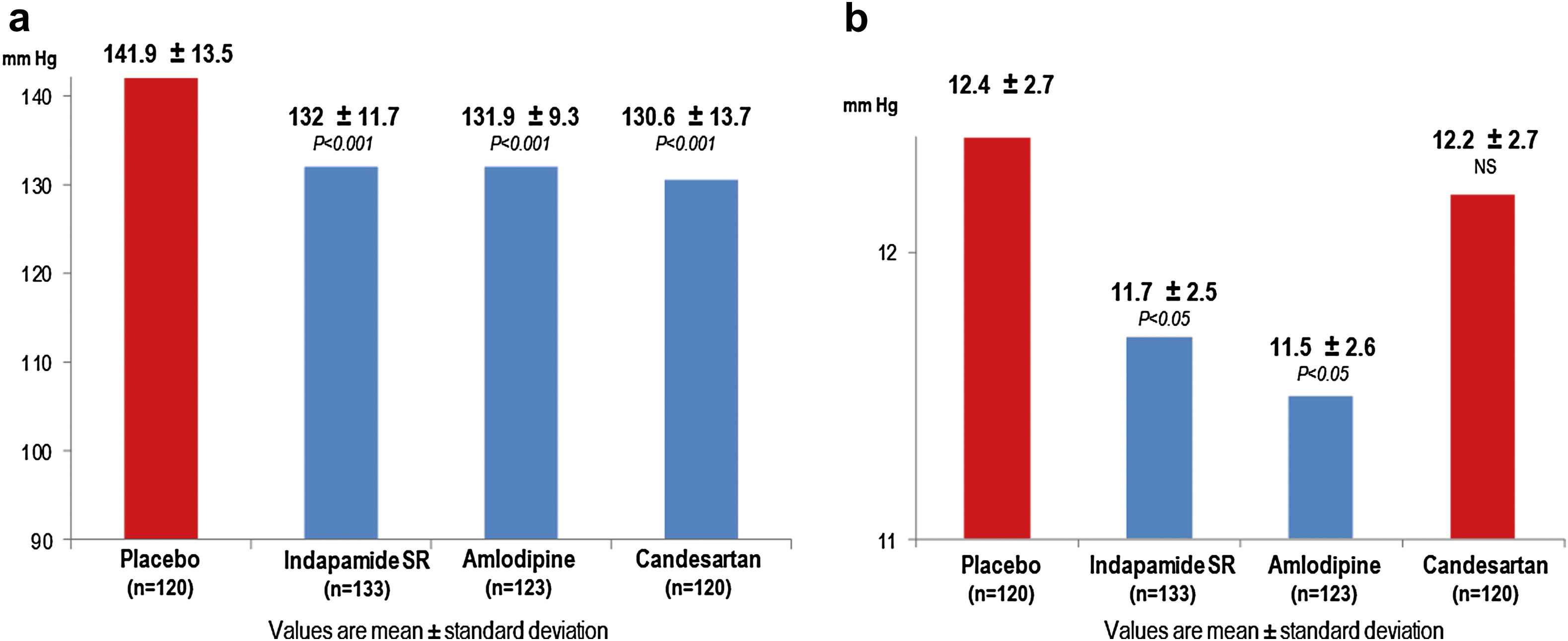
(a) Comparisons of mean 24-h systolic BP level after 3-month antihypertensive treatment. (b) Comparisons of 24-h systolic BP variability after 3-month antihypertensive treatment. P values are considered vs placebo.
Secondly we found that the major determinants of baseline systolic BPV were age, mean systolic BP, and heart rate variability (HRV). Thirdly, we found that amlodipine and indapamide SR decreased BPV by lowering BP or ameliorating the autonomic nervous system regulation or both. Their combination might help to optimize such properties.8,10
Conclusion
Clinical and experimental research indicates to day the interest of BP variability in the evaluation of cardiovascular risk. In anti-hypertensive treatment, reduction of BP variability may differ according to the antihypertensive agent which is used.
References
Cite this article
TY - JOUR AU - Michel E. Safar PY - 2011 DA - 2011/10/28 TI - BLOOD PRESSURE VARIABILITY AND ARTERIAL STIFFNESS JO - Artery Research SP - 119 EP - 121 VL - 5 IS - 4 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2011.10.001 DO - 10.1016/j.artres.2011.10.001 ID - Safar2011 ER -