
Methodological Consideration for Endothelial Function Assessment based on Bilateral Differences
 , Jonathan D. Keyser, Brock T. Jensen
, Jonathan D. Keyser, Brock T. Jensen- DOI
- 10.2991/artres.k.201031.001How to use a DOI?
- Keywords
- Bilateral considerations; arterial stiffness; endothelial function
- Copyright
- © 2020 Association for Research into Arterial Structure and Physiology. Publishing services by Atlantis Press International B.V.
- Open Access
- This is an open access article distributed under the CC BY-NC 4.0 license (http://creativecommons.org/licenses/by-nc/4.0/).
1. INTRODUCTION
Examining the characteristics and responses of an individual’s vascular system is important for improving the early detection, prevention, and treatment of cardiovascular disease. For example, applanation tonometry is a common means of assessing arterial stiffness, with precise standards established for measurement [1]. Previous studies have examined potential differences in arterial stiffness between arms [2–5], with conflicting findings. Further, while the assessment of arterial stiffness can provide a snapshot of vascular health at rest, information on dynamic vascular function can be determined by assessing the change in Pulse Wave Velocity (PWV) in response to a condition of reactive hyperemia [6–16].
2. AIMS
The primary aim was to determine bilateral, simultaneous arterial stiffness and endothelial function using applanation tonometry in apparently healthy individuals.
3. METHODOLOGY
3.1. Study Design
Participants reported to the lab on two separate occasions (at similar times of day, at least 48 h between visits). Following consent, the first visit required all healthy participants to arrive fasted (3 h), and free of alcohol/caffeine consumption and exercise (24 h). Initial resting measures included standardized indices of anthropometry and a metabolic panel. Female participants scheduled visits during the early follicular phase of their menstrual cycle to minimize the effect of hormonal fluctuations on autonomic and vascular measures.
All vascular measures were performed during visit two. Following a 10-min, supine rest, bilateral BP measurements were determined through manual auscultation. Standard pulse sites at the carotid, femoral, and right/left radial arteries were precisely measured using a portable infantometer. Pulse wave velocity was recorded at rest between the carotid and femoral sensors (CFPWV), and simultaneously at rest between the carotid and both radial sensors (CRPWV RIGHT, CRPWV LEFT) using standard applanation tonometry (Complior Analyse, Alam Medical, Saint Quentin Fallavier, France). Subsequently, a 5-min circulatory arrest was induced via cuff inflation around the forearm to a supra-systolic pressure (~220 mmHg) after which a second series of simultaneous, bilateral carotid-radial PWV measurements were taken approximately 60-s post cuff release. Flow-mediated slowing of carotid-radial PWV post cuff release was used as a measure of peripheral vascular endothelial function [8,11,15,16]. Thus, the resulting difference between pre- and post-occlusion PWV was recorded as endothelial function (ENDO).
Demographic variables were assessed and reported as means and standard error of the mean. Paired t-tests were performed to determine demographic differences, and arm (right and left) differences in PWV and ENDO. An a priori alpha level of 0.05 was determined as an appropriate level of significance across all analyses.
4. RESULTS
Twenty-four individuals (10 male, 14 female) completed the requirements of the study. The average participant was 25 ± 6 years of age and had healthy cholesterol and glucose values. The average participant was at the upper end of the healthy category for Body Mass Index (BMI) (24.0 ± 3.2 kg/m2) and had waist circumference values below cutoffs for concern. Except for lower Systolic Blood Pressure (SBP) in females (54.4 ± 7.3 vs. 67.5 ± 12.8 bpm, p < 0.01), there were no significant differences in demographic variables based on sex (Table 1). Systolic blood pressure was not significantly different in the right and left arms when simultaneously measured (p > 0.05). Inter-arm blood pressure Difference (IAD), that is clinically significant (IAD ≥ 10 mmHg) was only observed in one subject. Significant correlations existed unilaterally between ENDO and subject demographics (Table 2).
| Males (n = 10) | Females (n = 14) | Total (n = 24) | |
|---|---|---|---|
| Age (years) | 27.1 ± 2.5 | 23.4 ± 1.4 | 24.9 ± 1.3 |
| WT (kg)** | 82.6 ± 3.3 | 67.7 ± 3.2 | 73.9 ± 2.7 |
| HT (cm)** | 181.0 ± 3.1 | 170.6 ± 2.3 | 175.0 ± 2.1 |
| BMI (kg/m2) | 25.3 ± 1.0 | 23.2 ± 0.8 | 24.1 ± 0.7 |
| LBM (kg)** | 70.9 ± 2.9 | 50.5 ± 1.5 | 59.0 ± 2.6 |
| WC (cm)** | 85.4 ± 2.5 | 75.6 ± 2.0 | 79.7 ± 1.8 |
| TC (mg/dL) | 181.4 ± 13.1 | 184.8 ± 9.2 | 183.4 ± 7.3 |
| LDL (mg/dL) | 107.7 ± 10.4 | 98.4 ± 10.5 | 102.3 ± 7.3 |
| HDL (mg/dL)* | 51.8 ± 3.6 | 67.6 ± 4.6 | 61.0 ± 3.4 |
| LDL/HDL | 2.2 ± 0.3 | 1.6 ± 0.2 | 1.8 ± 0.2 |
| TG (mg/dL) | 110.5 ± 21.6 | 100.2 ± 14.4 | 104.5 ± 11.8 |
| GLU (mg/dL) | 94.3 ± 2.2 | 91.2 ± 2.6 | 92.5 ± 1.7 |
| RHR (bpm) | 60.2 ± 4.8 | 64.4 ± 3.2 | 62.6 ± 2.6 |
| SBP (mmHg)* | 126.3 ± 3.1 | 117.6 ± 1.9 | 121.2 ± 1.9 |
| DBP (mmHg) | 74.1 ± 2.9 | 74.4 ± 2.1 | 74.3 ± 1.7 |
| IAD (mmHg) | 4.8 ± 1.2 | 3.1 ± 0.6 | 3.8 ± 0.6 |
| CFPWV (m/s) | 5.8 ± 1.2 | 6.0 ± 0.8 | 5.9 ± 0.9 |
| CRPWV RIGHT (m/s) | 8.3 ± 0.4 | 8.3 ± 0.3 | 8.3 ± 0.3 |
| CRPWV LEFT (m/s) | 7.2 ± 0.4 | 7.7 ± 0.3 | 7.5 ± 0.2 |
| CRPWV DIFF (m/s) | 1.1 ± 0.3 | 0.6 ± 0.3 | 0.8 ± 0.3 |
p < 0.05,
p < 0.01.
All data are presented as mean ± SD.
WT, weight; HT, height; BMI, body mass index; LBM, lean body mass; WC, waist circumference; TC, total cholesterol; LDL, low density lipoprotein; HDL, high density lipoprotein; TG, triglycerides; GLU, blood glucose; RHR, resting heart rate; SBP, systolic blood pressure; DBP: diastolic blood pressure.
Subject demographics
| Males (n = 10) | Females (n = 14) | |||||||
|---|---|---|---|---|---|---|---|---|
| ENDORIGHT | ENDOLEFT | ENDORIGHT | ENDOLEFT | |||||
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | |
| Age | −0.17 | 0.62 | 0.45 | 0.19 | −0.11 | 0.7 | 0.17 | 0.55 |
| BMI | 0.62 | 0.05* | 0.26 | 0.45 | −0.42 | 0.13 | −0.06 | 0.82 |
| WC | 0.6 | 0.06 | 0.31 | 0.36 | −0.48 | 0.08 | −0.18 | 0.51 |
| TC | −0.28 | 0.42 | −0.37 | 0.28 | −0.42 | 0.12 | −0.43 | 0.12 |
| HDL | 0.39 | 0.25 | −0.14 | 0.69 | 0.24 | 0.39 | 0.48 | 0.07 |
| LDL | −0.44 | 0.19 | −0.27 | 0.43 | −0.48 | 0.07 | −0.49 | 0.07 |
| LDL/HDL | −0.42 | 0.22 | −0.18 | 0.61 | −0.43 | 0.11 | −0.5 | 0.06 |
| TG | −0.11 | 0.75 | −0.33 | 0.35 | 0.01 | 0.98 | −0.22 | 0.44 |
| GLU | 0.1 | 0.78 | −0.09 | 0.79 | −0.1 | 0.73 | 0.26 | 0.36 |
| RHR | 0.57 | 0.07 | −0.29 | 0.41 | 0.58 | 0.02* | 0.18 | 0.53 |
| DP | 0.15 | 0.67 | −0.06 | 0.86 | 0.58 | 0.02* | 0.09 | 0.74 |
| SBP | 0.48 | 0.15 | −0.12 | 0.73 | 0.23 | 0.41 | −0.27 | 0.34 |
| SBPc | 0.73 | 0.01** | −0.44 | 0.19 | 0.3 | 0.29 | −0.3 | 0.29 |
| DBP | 0.25 | 0.48 | 0.09 | 0.78 | 0.18 | 0.51 | 0.17 | 0.56 |
| PP | 0.76 | 0.01** | 0.02 | 0.93 | 0.02 | 0.92 | 0.41 | 0.14 |
Significant correlation
p < 0.05;
p < 0.01.
BMI, body mass index; WC, waist circumference; TC, total cholesterol; HDL, high density lipoprotein; LDL, low density lipoprotein; TG, triglycerides; GLU, blood glucose; RHR, resting heart rate; DP, double product; SBP, systolic blood pressure; SBPc, central systolic blood pressure; DBP, diastolic blood pressure; PP, pulse pressure.
Correlations between ENDO and demographics for males and females
Bilateral carotid-radial PWV and ENDO were measured simultaneously. All PWV tolerance values for the left and right arms were ≥95%. Due to the short half-life of nitric oxide during the collection of ENDO, an a priori level of ≥90% was determined as an acceptable level of tolerance for left and right arms. Our lab demonstrated the following coefficients of variation in our applanation tonometry measures: carotid-femoral—3.5%, carotid-radial—5.7%, and FMD—9.6% and had PWV and ENDO values above the acceptable limit for both the right and left arm [6,7]. Specifically, the average tolerance for ENDO for the right and left arms were 95.1 ± 2.0% and 95.0 ± 2.0%, respectively. PWV was 10% greater in the right arm when compared to the left arm (Figure 1; CRPWV RIGHT = 8.3 ± 0.3 vs. CRPWV LEFT = 7.5 ± 0.2 m/s; CRPWV DIFF = 0.8 ± 0.3, p < 0.05). Similarly, ENDO was 8% greater in the right arm when compared to the left arm (Figure 2; ENDORIGHT = 7.8 ± 0.2 vs. ENDOLEFT = 7.2 ± 0.2; ENDODIFF = 0.6 ± 0.1; p < 0.05).
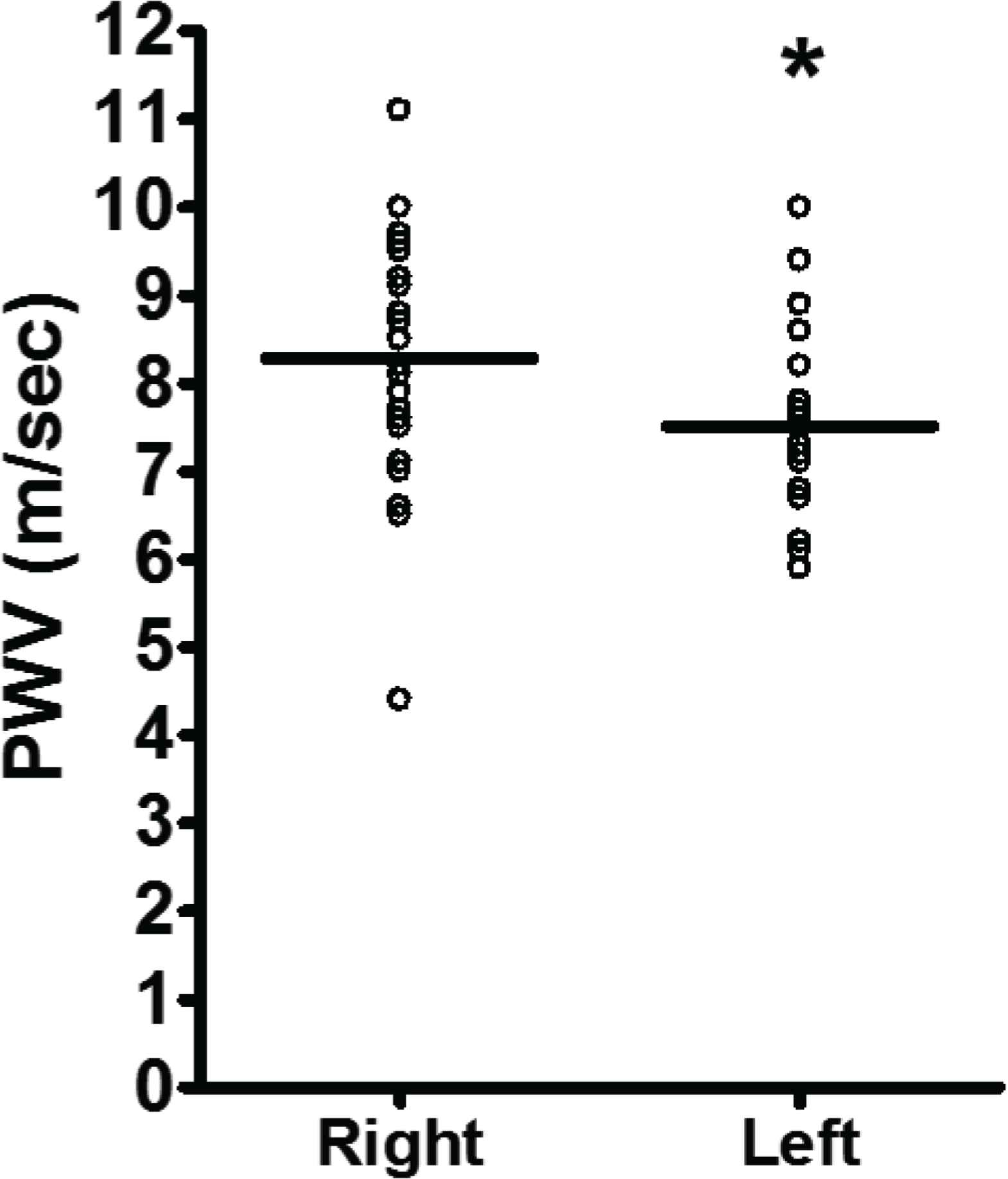
Carotid-radial PWV measured simultaneously in right and left arms. Data are mean ± SD. Significant difference from right arm *p < 0.05.
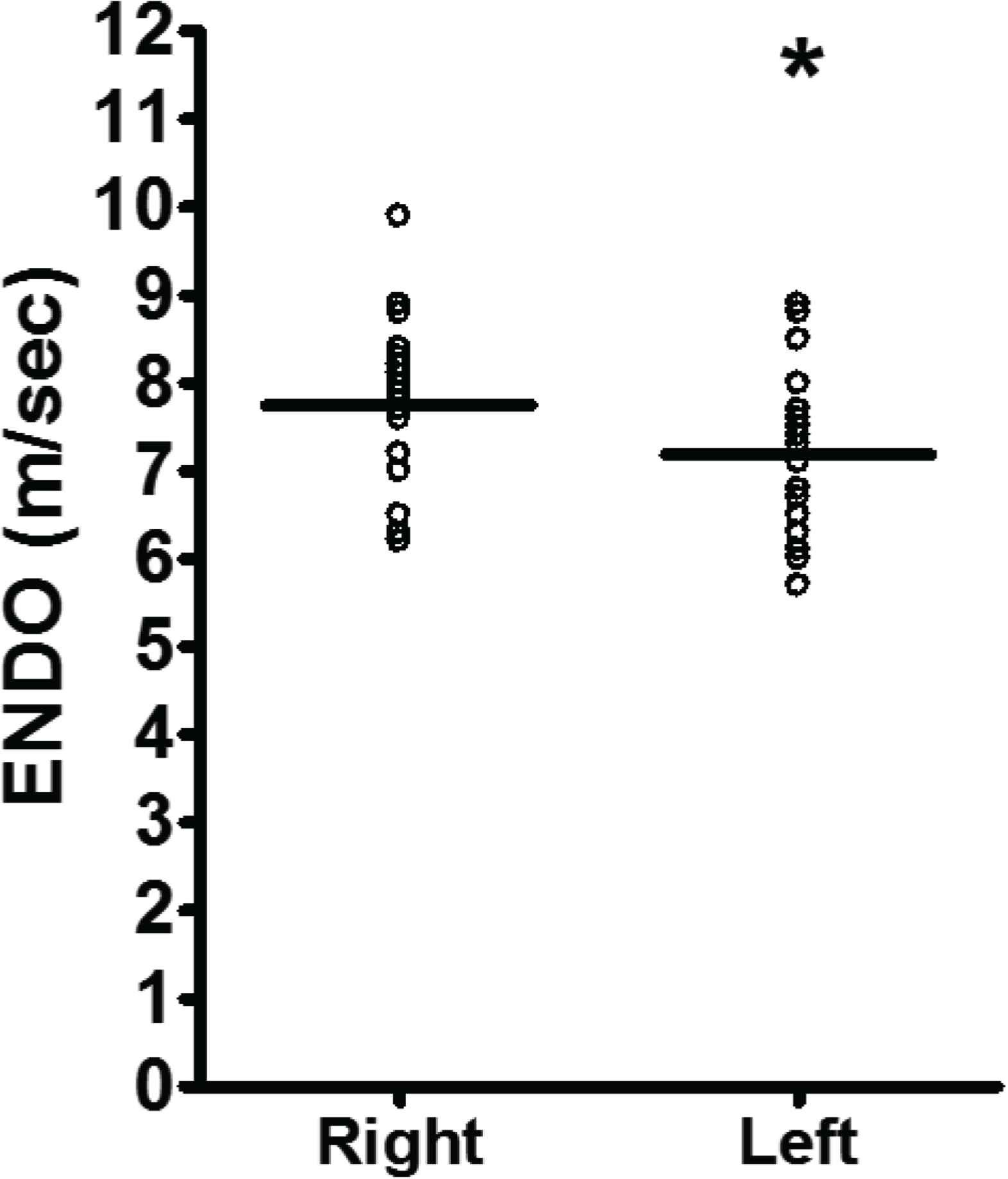
Carotid-radial ENDO measured simultaneously in right and left arms. Data are mean ± SD. Significant difference from right arm *p < 0.05.
5. CONCLUSION
Blood pressure measurement has specific standards [17], including bilateral considerations, though there is a paucity of literature related to the bilateral measurement of PWV or ENDO. Previous studies have reported no differences in bilateral brachial waveforms [3–5]. Martin et al. [2], however, observed inter-arm differences in arterial stiffness in line with our study.
Bilateral endothelial function has not been previously quantified. In the current investigation, ENDO was different between arms and was not dependent on hemodynamic or demographic variables. Interestingly, the relationship between endothelial function measured in each arm and pressure measures were contrasting. Additionally, the observed relationships, while physiologically reasonable given the higher arm PWV and ENDO measures, were varied between males and females. Further investigation designed to specifically understand these potential mechanisms, and sex differences, may be warranted. The possibility exists that these observed differences are simply due to the anatomy of the arterial tree as proposed with inter-arm blood pressure differences [18]. To the best of our knowledge, bilateral anatomical differences have not been precisely quantified in young, apparently healthy individuals, and while this proposed mechanism has not been explicitly addressed in the literature, consideration could be given to simulation modeling [19] to provide insight into an anatomical or physiological rationale for arterial segment differences. Further, studies evaluating the bilateral PWV and ENDO relationship in aged and clinical populations with known pathology may be valuable as age associated increases in vascular resistance and/or asymmetrical vascular disease likely contribute differing PWV characteristics.
The present study points to the importance of measuring anatomical (i.e., PWV) and physiological (i.e., ENDO) vascular measures bilaterally, as differences may exist between arms. In line with established recommendations related to the bilateral measurement of blood pressure, it may be prudent to measure PWV/ENDO bilaterally and make important decisions regarding the detection, prevention, and treatment of cardiovascular disease using the results from the higher arm.
CONFLICTS OF INTEREST
The authors declare they have no conflicts of interest.
AUTHORS’ CONTRIBUTION
MEH and BTJ were equally responsible for the literature search, study design, data collection, data analysis, and manuscript writing and revision. JDK contributed to data analysis, manuscript writing, and manuscript revision.
Footnotes
REFERENCES
Cite this article
TY - JOUR AU - Michael E. Holmstrup AU - Jonathan D. Keyser AU - Brock T. Jensen PY - 2020 DA - 2020/11/09 TI - Methodological Consideration for Endothelial Function Assessment based on Bilateral Differences JO - Artery Research SP - 47 EP - 50 VL - 27 IS - 1 SN - 1876-4401 UR - https://doi.org/10.2991/artres.k.201031.001 DO - 10.2991/artres.k.201031.001 ID - Holmstrup2020 ER -