
24-h ambulatory pulse wave velocity and central blood pressure in type 2 diabetes
- DOI
- 10.1016/j.artres.2014.04.004How to use a DOI?
- Keywords
- Ambulatory; Pulse wave velocity; Central blood pressure; Augmentation index; Brachial cuff; Pulse wave analysis; Arteriograph; Diabetes
- Abstract
Background: Pulse wave analysis from a brachial cuff permits ambulatory measurements of pulse wave velocity (PWV) and central blood pressure parameters. The diurnal variation of PWV in type 2 diabetes is unknown.
Methods: We evaluated the Arteriograph24 which is a brachial cuff based equipment for estimating PWV and central blood pressure data without the use of a transfer function, in 22 type 2 diabetic patients, who had two 24 h measurements performed.
Results: The mean number of valid day time and nighttime measurements were 29 (range 16–50) and 18 (11–25), respectively. 21 patients had at least one qualifying report. Nighttime PWV was significantly lower than during the day (9.1 vs. 9.7 ± 0.8 mm/s, p < 0.01). Systolic aortic blood pressure was 6 mmHg lower than brachial blood pressure in the day time (p < 0.01) and 4 mmHg lower during the night (p < 0.05). Each single measurement was standardized with the 24 h average as reference thus generating data from 1004 paired observations. The standardized PWV correlated with standardized values of heart rate (r = 0.24, p < 0.001) and systolic aorta blood pressure (r = 0.20, p < 0.001). A stepwise multiple regression model with standardized pulse wave velocity as dependent variable included standardized heart rate, systolic aorta blood pressure and a dummy variable for day/night status (R2 = 0.091, p < 0.001).
Conclusion:The Arteriograph24 is applicable for research purpose. PVW in type 2 diabetes is modestly reduced during the night. The intraindividual variation of heart rate contributed independently to the variation of PWV.
- Copyright
- © 2014 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Arterial stiffness is believed to reflect the cumulated arteriosclerotic “load” and is thus relatively independent of the actual presence of risk factors which can be modified on short term basis by pharmacological treatment or change in lifestyle.1 Arterial stiffness assessed by measurement of pulse wave velocity (PWV) has been shown to predict cardiovascular events independently of known risk factors both in the general population2 and different high risk populations including type 2 diabetes.3–6
The gold standard for assessing PWV is direct measurement of the traveled distance divided by the time. Traditionally this method depends on tonometry of two arteries which requires some technical skills. The Arteriograph offers an indirect, easily obtained assessment of PWV which is based on analysis of the pulse wave from a brachial cuff inflated to supra-systolic blood pressure (BP) values for a few seconds. The time lag between the first and second (reflected) systolic peak is thought to reflect the time the pulse wave takes to travel from the ascending aorta to the aortic bifurcation and back.7 Although the theoretical principle of a “fixed” reflection point has been disputed,8–10 several studies have shown that the Arteriograph obtain values close to those obtained by established direct methods7,11,12 and these are indeed very close to PWV values obtained in a study calculating travel distance and time based on MR evaluation of the aorta.13 More importantly, a recent prospective study using the Arteriograph in a low risk population has demonstrated, for the first time that cardiovascular events can be predicted over and above other well-known cardiovascular risk factors by indirectly measured PWV.14
In addition, the Arteriograph offers an estimate of the central aortic augmentation index (AIXao) and systolic aorta BP (SYao) based on an empiric relation between brachial AIX and invasively obtained AIXao,15 which has been compared to other indirect techniques12 and validated by comparison with invasive measurements in patients with type 2 diabetes.16
Twenty four hour ambulatory measurement of brachial BP is a well-established clinical tool for diagnosing hypertension and evaluating the effect of antihypertensive treatment. Ambulatory BP improves prediction of cardiovascular events and the particular importance of high nighttime BP has been demonstrated in several studies.17
The availability of brachial pulse wave analysis by small monitors has recently opened for a new interesting field in cardiovascular research, namely ambulatory assessment of pulse wave velocity and central aortic blood pressure.
Our aim of this pilot study was to evaluate the applicability and reproducibility of the Arteriograph24 equipment for ambulatory assessment of PWV, SYao and the central aortic augmentation index. In addition, we wished to obtain data regarding the diurnal variation of these parameters in type 2 diabetic patients.
Methods
Type 2 diabetes patients visiting the outpatient clinic at Regional Hospital Silkeborg, Denmark, were consecutively invited to participate. 25 patients were asked to perform two 24 h ambulatory measurements and 22 gave written and informed consent. The study was approved by the Central Denmark Region Committees on Health Research Ethics and by the Danish Data Protection Agency and registered in ClinicalTrials.govID (NCT01812811).
The brachial BP was measured simultaneously three times on both arms using Microlife WatchBP Office (Microlife AG, Switzerland). During measurements the patients were placed in a specially designed chair with adjustable armrests, securing the position of the upper arms at heart level. The average BP of each arm was given and determined which arm should be used for the Arteriograph24 (Tensiomed, Budapest, Hungary) measurements. If the difference in BP between the arms was less than 10 mmHg the patient could choose which arm to use, otherwise the arm with the highest BP was used. All chose the non-dominant arm for measurement. The brachial blood pressure measurements are based on the TensioDay device (TensioMed, Budapest, Hungary) which has previously been validated.18
The appropriate cuff for Arteriograph24 measurements was chosen according to the manufactures specifications. The guide is an integrated part of the individual programming. For arm circumference ≥34 cm cuff no. 1 was used (bladder dimensions 34 × 8 cm), for arm circumference 26–33 cm cuff no. 2 was used (26 × 8 cm) and for arm circumference 18–25 cm cuff no. 3 was used (18 × 6 cm).
Before attaching the Arteriograph24, the distance from the jugular notch to the pubic symphysis was measured using a caliper whilst the patient was in a supine position.
After the Arteriograph24 was programmed, three manual measurements were performed. Only information on BP and heart rate is visible on the Arteriograph24 display. After the manual measurements patients were instructed to keep the Arteriograph24 on for twenty four hours before removing. It was emphasized that the arm should be held still during measurements.
Arteriograph24 was programmed to perform measurements every 20 min. After first inflation, deflation and calculation of brachial blood pressure, the cuff is immediately inflated again to a value 35 mmHg above the systolic BP for approximately 6 s. If the obtained suprasystolic pulse wave fulfills the built in quality criteria, calculations of PWV, AIXao and SYao is performed by the software. These values cannot be seen directly on the display but must await download.
Night and day period was based on the patient information of time for going to bed and rising in the morning. Daytime and nighttime averages were calculated as the arithmetic mean of all values in the respective period and the 24 h value was weighted according to the length of the day and night period.
The criterion for a successful 24 h measurement was ≥14 PWV values available in the daytime and ≥7 values in the nighttime. This is an adoption of the minimum criteria recommended for ambulatory measurement of brachial BP at the time the study was planned.19 Blood samples were obtained for measurement of glycated hemoglobin (HbA1c), non-fasting fractioned lipid profile and p-creatinine. Three early morning urines were collected for measurement of albumin/creatinine ratio. The Tensiomed software version 2.4.01 (released 14.02.2012) was used primarily. Measurements that did not lead to calculated values despite the presence of a pulse pressure curve were reevaluated with the version 2.5.0 (released 01.10.2013).
Statistical analysis
Continuous variables are presented as mean ± SD and range. Normal distribution was tested by Q–Q plots. Data on the diurnal variation and results from day 1 and 2 are compared with student t test for paired observation. A two tailed p value <0.05 was considered statistical significant and the 95% confidence interval (CI) for the difference are given. Reproducibility is given as the standard deviation of the difference (SDD) between day 1 and day 2. Bivariate correlations were calculated as the Pearson correlation coefficient r. We standardized individual PWV values in order to describe the possible covariation with standardized values of MAP, SYao and heart rate (HR), irrespective of the actual level of the parameters. For each patient the result of every single measurement of PWV, MAP, SYao, HR and AIXao was standardized with the 24 h average of the component as the reference value 100 units. Multiple linear regression was performed as stepwise selection procedure with standardized PWV as dependent variable and the following independent variables: age, sex, standardized HR, standardized SYao, and a dummy variable indicating if a value were obtained in the day- or nighttime. The statistical software program SPSS version 18.0 was used.
Results
Of the 22 participating patients 17 patients had an acceptable 24 h PWV report for the first ambulatory measurement. Failures were due to absence of signal in two patients and in three patients the number of measurements were less than 14 in the daytime or less than 7 during the night. In the second measurement 17 patients had an acceptable 24 h PWV report; no signal was obtained from three patients and in one the signals disappeared after three hours due to low battery status. This case and the examples with no obtained pulse pressure curve may in part be operator dependent (problems with cuff placement). At the second measurement one patient did not qualify due to a low number of measurements. Overall 44 attempts resulted in 34 reports that fulfilled the quality criteria (77%). If the failures (n = 5) which could be operator dependent is disregarded, the success rate is 17/39 = 87%.
13 patients had acceptable reports for both measurements and their first report was chosen for evaluation of the diurnal variation. In 4 patients only the first measurement qualified and in 4 patients only the second measurement. Hence 21 patients contributed to the study of the diurnal variation of PWV and SYao. The clinical data are shown in Table 1 which also gives a detailed description of the glycemic, antihypertensive and antithrombotic treatment as well as the history of previous cardiovascular events. The mean brachial circumference was 32.0 ± 3.2 cm (25.0–39.0) and the mean jugular-symphysis distance 53.9 ± 2.8 cm (49.0–59.0).
| Sex (male/female) | 18/3 (86, 14%) |
| Age (years) | 65 ± 7 (52–78) |
| Diabetes duration (years) | 11.6 ± 6.8 (1–23) |
| Body mass index (kg m−2) | 30.8 ± 4.4 (25.5–41.5) |
| HbA1c (mmol/mol) | 60.4 ± 17.6 (36–101) |
| Total cholesterol (mmol/l) | 3.7 ± 0.8 (2.7–5.6) |
| LDL cholesterol (mmol/l) | 1.9 ± 0.6 (1.1–3.3) |
| p-creatinine (micromol/l) | 100 ± 30 (50–165) |
| Normo/micro/macroalbuminuria (number) (<30/30–300/> 300 mg/g) |
11/8/2 (52/38/10%) |
| Smoking (no/yes/previous) | 7/4/10 (33/19/48%) |
| Previous cardiovascular events | 13 (62%) |
| Insulin | 15 (71%) |
| Metformin | 14 (33%) |
| Glucagon like peptide 1 antagonist | 5 (24%) |
| Sulfonylurea | 2 (10%) |
| Statin | 16 (76%) |
| Antihypertensive treatment | 20 (95%) |
| Number of antihypertensive drugs (0/1/2/3/4/5) | 1/1/9/2/5/3 (5/5/43/10/24/14%) |
| ACE or ARB | 19 (90%) |
| Thiazide or loop diuretic | 15 (71%) |
| Spironolactone | 6 (29%) |
| Ca antagonist | 9 (43%) |
| Beta- blocker | 9 (43%) |
| Alpha blocker or moxonidin | 2 (10%) |
Values are mean ± SD (range) or numbers (fraction %).
Clinical characteristics of type 2 diabetic patients.
The number of measurements during day- and nighttime, the length of the period and the number of hours with at least one valid measurement of PWV as well as central aorta data are shown in Table 2. The success rate was higher during the night (75%) than in the daytime (57%, p < 0.01). Overall close to 90% of the hours had at least one successful measurement of PWV and central aorta data.
| Day | Night | |
|---|---|---|
| Duration (min) | 980 ± 66 (881–1110) |
460 ± 66 (330–559) |
| Attempted PWV measurements (number) | 49.5 ± 4.2 (43–60) |
23.8 ± 3.5 (16–29) |
| Successful PWV measurements (number) | 28.5 ± 9.4 (16–50) |
17.5 ± 4.3 (11–25) |
| Success rate (%) | 57.2 ± 16.4 (34.0–96.2) |
74.6 ± 17.4 (40.7–100.0) |
| Hours (number) | 14.3 ± 1.5 (12–17) |
7.2 ± 1.3 (5–9) |
| Hours with at least one successful PWV measurement (number) | 12.1 ± 2.6 (8–17) |
6.9 ± 1.3 (5–9) |
| Fraction of hours with at least one successful PWV measurement (number) | 84.6 ± 14.6 (53–100) |
95.8 ± 9.2 (63–100) |
Values are mean ± SD (range).
Performance of the Arteriograph24 monitor.
PWV at night was slightly but significantly lower than daytime PWV (difference 0.6 m/s; CI (0.3–0.9, p < 0.01) (Table 3). SYao was 6 mmHg lower than brachial systolic BP in the day time (p < 0.01) and 4 mmHg lower in the nighttime (p < 0.05). Daytime AIXao was not statistically significant from nighttime AIXao (23 ± 9% vs 25 ± 12%, CI of the difference: −5.0–0.6%, p = 0.12).
| PWV (m/s) | Systolic brachial (mmHg) | Systolic aorta (mmHg) | Brachial - aorta (paired t-test) | AIXao (%) | MAP brachial (mmHg) | Diastolic brachial (mmHg) | Heart rate (beats/min) | |
|---|---|---|---|---|---|---|---|---|
| Daytime Arteriograph | 9.7 ± 0.8 (7.6–11.2) |
134 ± 14 (111–167) |
127 ± 13 (105–157) |
6.4 ± 6.0 p < 0.001 CI (3.7–9.2) |
23 ± 9 (3–45) |
95 ± 10 (81–121) |
76 ± 9 (62–98) |
76 ± 9 (61–89) |
| Nighttime Arteriograph | 9.1 ± 1.2 (6.1–10.7) |
123 ± 16 (99–163) |
118 ± 18 (95–156) |
4.3 ± 6.5 p < 0.01 CI (1.3–7.3) |
25 ± 12 (6–51) |
85 ± 12 (71–110) |
66 ± 10 (55–84) |
70 ± 10 (50–91) |
| 24 h Arteriograph | 9.5 ± 0.9 (7.2–11.2) |
130 ± 14 (108–166) |
124 ± 14 (102–157) |
5.7 ± 5.9 p < 0.001 CI (3.1–8.4) |
24 ± 10 (4–46) |
92 ± 11 (78–118) |
73 ± 9 (60–94) |
74 ± 9 (59–88) |
| Night/day % Arteriograph | 94 ± 8 (80–107) |
92 ± 6 (81–101) |
93 ± 7 (79–104) |
−1.2 ± 2.7 p = 0.07 CI (−2.7 to 0.2) |
111 ± 35 (70–193) |
89 ± 7 (77–100) |
87 ± 8 (71–99) |
92 ± 9 (77–107) |
Values are mean ± SD (range) and 95% confidence interval (CI).
Results of 24 h ambulatory monitoring (n = 21).
The standardization of individual measurements for the 21 patients provided 1004 paired values to describe the intraindividual relative variation of PWV, AIXao, SYao, mean arterial pressure (MAP) and HR (Fig. 1). The standardized PWV (STDPWV) correlated with standardized HR (STDHR), standardized SYao (STDSYao) and standardized MAP (STDMAP) (r = 0.24, r = 0.20, r = 0.16 respectively, p < 0.001 for all). Both STDMAP (r = 0.35) and STDSYao (r = 0.17) correlated with STDHR (p < 0.001). A multiple stepwise regression model with STDPWV as dependent variable included STDHR (beta coefficient = 0.28/unit, p < 0.001) STDSYao (beta = 0.18/unit, p < 0.001), and dichtomized day/night status (beta = −2.9 for night, p < 0.01) as independent variables but excluded age and sex (R2 = 0.09, p < 0.001). If STDMAP replaced STDSYao as independent variables only STDHR and day/night status contributed significantly to the model. Standardized AIXao correlated negatively with STDHR (r = −0.31, p < 0.001).
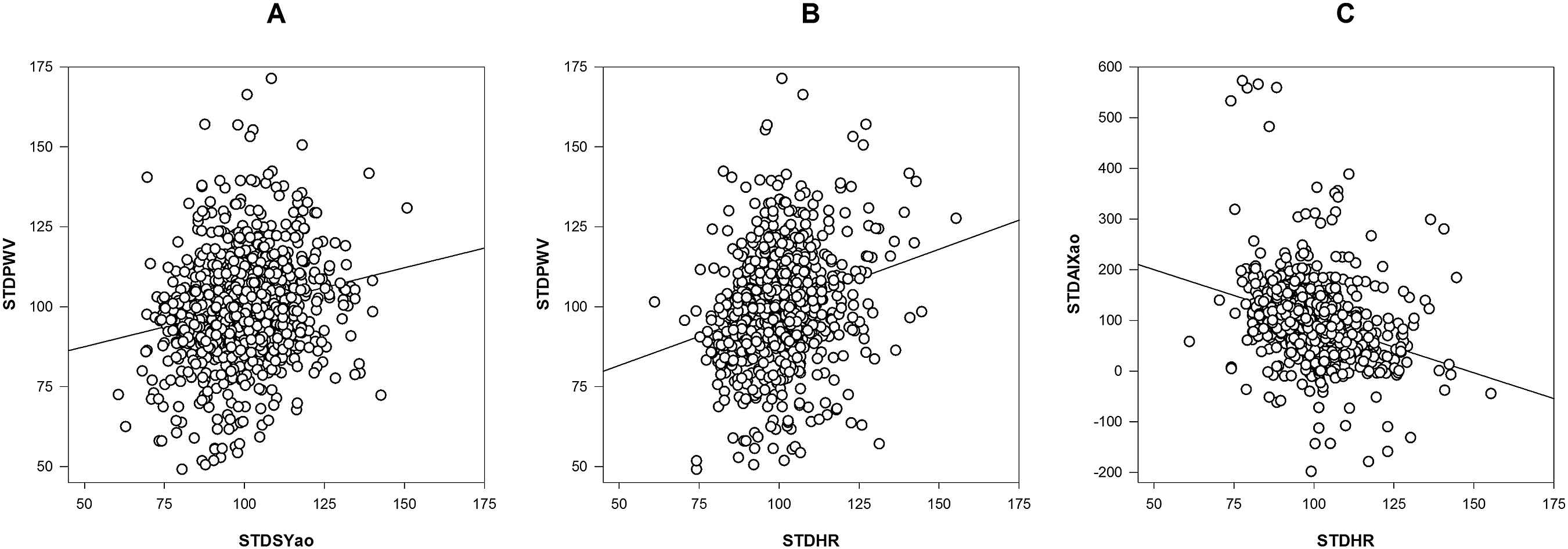
Scatter plot of standardized (STD) values of (A) PWV and SYao (B) PWV and HR (C) AIXao and HR obtained from ambulatory recordings in 21 type 2 diabetic patients (n = 1004 paired observations, after omitting two PWV and one AIXao outliers). Each measurement is standardized to a value 100 units corresponding to the 24 h average for each component for each patient.
The reproducibility part of the study was based on 13 patients with two acceptable measurements performed with a mean interval of 14 days (range 6–28). Visual inspection of a plot depicting the difference between PWV, AIXao and SYao showed no influence of the mean value (figure not shown). There was no statistical significant difference between day 1 and day 2 for any of the parameters (Table 4).
| Day 1 | Day 2 | Day1-day 2 | SDD | |
|---|---|---|---|---|
| Brachial systolic day (mm Hg) | 132.2 ± 12.3 | 132.5 ± 9.4 | −0.3; p = 0.88 | 7.0 |
| Brachial systolic night (mm Hg) | 122.0 ± 14.9 | 123.2 ± 12.3 | −1.2; p = 0.57 | 7.1 |
| Brachial systolic 24 h (mm Hg) | 129.1 ± 12.7 | 129.7 ± 10.2 | −0.6; p = 0.78 | 6.9 |
| Number of PWV measurements day | 30.4 ± 10.0 | 29.7 ± 8.0 | 0.7; p = 0.76 | 7.8 |
| Number of PWV measurements night | 17.9 ± 4.3 | 17.9 ± 4.7 | 0.0; p = 1.0 | 4.9 |
| AIXao day (%) | 22.8 ± 11.1 | 21.9 ± 7.7 | 0.8; p = 0.64 | 6.4 |
| AIXao night (%) | 24.5 ± 14.1 | 25.5 ± 12.5 | −0.9; p = 0.74 | 9.8 |
| AIXao 24 h (%) | 23.3 ± 11.7 | 23.0 ± 8.8 | 0.3; p = 0.89 | 6.6 |
| Aorta systolic day (mm Hg) | 124.9 ± 11.9 | 125.2 ± 10.0 | −0.3; p = 0.87 | 6.8 |
| Aorta systolic night (mm Hg) | 117.4 ± 16.2 | 118.5 ± 13.6 | −1.2; p = 0.51 | 6.1 |
| Aorta systolic 24 h (mm Hg) | 122.7 ± 12.9 | 123.2 ± 10.9 | −0.5; p = 0.76 | 6.0 |
| PWV day (m/s) | 9.6 ± 0.9 | 9.9 ± 0.9 | −0.3; p = 0.40 | 1.0 |
| PWV night (m/s) | 9.0 ± 1.3 | 9.4 ± 1.2 | −0.4; p = 0.34 | 1.6 |
| PWV 24 h (m/s) | 9.4 ± 1.0 | 9.7 ± 0.9 | −0.3; p = 0.34 | 1.1 |
Values are mean ± SD unless other specified.
Results of test- retest of 24 h ambulatory monitoring of PWV and central aortic BP data (n = 13).
Discussion
We have demonstrated a diurnal variation of PWV in type 2 diabetes with nighttime PWV reduced to about 94% of the day time values. Even type 2 diabetic patients with short diabetes duration have higher PWV (9.3 m/s ± 2.0) (measured in the clinic) than healthy controls (8.0 m/s ± 1.6)20 and an even larger difference (13.9 vs. 11.5 m/s) was found in a study comparing non-diabetic subjects with diabetic patients with presumably longer diabetes duration.21 In a study of 83 mainly healthy hospital staff members a slight reduction of PWV was noted during nighttime when ambulatory monitoring was performed with the Mobil-O-Graph monitor.22 However this reduction was not quantified. To our knowledge no previous studies have reported on the diurnal variation of PWV in diabetic patients.
The principle of indirect measurement of PWV from a brachial pulse wave has been validated only in subjects resting in supine position. It is unknown if movements during daily life activities could introduce artifacts or a change in the hypothetical wave reflection point. In addition it can be speculated if the change per se from supine (during the night) to upright position (in the day) affects PWV due to the hydrostatic effect on blood pressure in the vertical aorta column. We are not aware of any study comparing PWV in supine and upright position by direct methods.
The SYao was significantly lower (about 6 mmHg) than the brachial BP in the daytime. This relatively low central to peripheral blood pressure amplification is most likely due to stiff arteries in the diabetic patients. We have previously reported an even lower central to peripheral amplification (about 1 mmHg) in type 2 diabetic patients with similar age (65 years) and diabetes duration (9 years) who probably had more advanced arteriosclerotic lesions because the patients were recruited for participation in an invasive validation study among candidates for coronary angiography.16 In contrast the brachial –central BP difference in diabetes was reported much higher (13 mmHg) by the Anglo-Cardiff trial using the Sphygmocor.23 This may depend on methodological differences between the estimates of central BP obtained by tonometry and a transfer function versus estimates based on pulse wave analysis obtained from a brachial cuff.
The plot of STDPWV values showed huge scatter, probably due to analytical errors and only about 3.8% of the variation could be explained by changes in STDSYao. The influence of HR on PWV has been questioned by some researchers.24 We found that both STDSYao and STDHR were included in a multiple regression model with STDPWV as dependent variable. The contribution of a dummy variable for nigh/day status may be explained as the influence of sympatovagal balance. It is a novel finding that the variation in daily life MAP did not contribute to the variation in PWV when changes in HR were accounted for. In a cross sectional study interindividual PWV variation was related to MAP levels in non-diabetic subjects but not in diabetic patients,21 however these observations cannot directly be compared to our study of the within-patient relation between variations in PWV and MAP. The influence of HR on PWV has been described previously in pace studies (with no change in BP)25 and this finding is independent of the method used to estimate PWV, whether direct methods26 or indirect methods as used in this study. The pathophysiological mechanisms underlying the association between PWV and HR could be changes in the elastic properties of the arterial wall, but the explanation remains essentially obscure.26 It is reassuring that standardized AIXao assessed with a brachial cuff method is negatively correlated with standardized heart rate as expected from invasive measurements of AIXao.27 We noticed a tendency to higher AIXao during the night which may be due to the lower nocturnal heart rate. A significant nocturnal increase of AIXao, which disappeared after correction to a standard heart rate of 75, was found in the Mobil-O-Graph study.22
Even though our minimum criteria for a qualifying 24 h report was not very ambitious, only 77% of the reports were acceptable, and among these reports the fraction of successful measurements of PWV were between 57% (daytime) and 75% (nighttime). Due to the sampling frequency of a measurement every 20 min we obtained a satisfactory result with nearly 90% of all hours represented with at least one valid measurement. Failed measurements may primarily be due to motion errors since the success rates were higher at night. The rate of good quality ambulatory PWV measurements with the Mobil-O-Graph has been reported between 74%22 and 83%28 for a 24 h period.
We believe that the reports without any pulse wave signal are due to problems with the cuff. The equipment seems sensitive to correct placement and tightening of the cuff. The cases with no signals might have been avoided if it had been possible to obtain real time results of PWV and central BP data displayed on the monitor. This would allow for new attempts with a different cuff position and tightening before the patient left the office.
The reproducibility part of our study should be interpreted cautiously because of the low number of participants (n = 13). The standard deviation of the difference (SDD) for two measurements of 24 h systolic aorta BP was comparable with the SDD for 24 h brachial systolic BP. The SDD for two 24 h measurements of PWV was 1.1 m/s which is comparable with results from other studies measuring PWV by direct methods in the office, including a study in type 2 diabetic patients reporting SDD values ranging from 0.7 to 2.2 m/s.29–33 We had expected a lower value of SDD for ambulatory PWV monitoring because of the number of measurements (app. 48) during a 24 h period rather than a single or double measurement usually performed in the office. In the reproducibility study using the Mobil-O-Graph the SDD of PWV was very low 0.09 m/s based on app. 57 measurements per 24 h period in a study with 30 subjects.28 Part of the explanation may be the visual inspection of all blood pressure curves and deletion of measurements if the brachial waveforms were judged of poor quality.28 We have not performed any post measurement editing before calculating PWV despite some results seemed obvious outliers, since no accepted criteria for editing exist so far. In this respect our data handling follows recommendations for ambulatory measurements of brachial BP which discourage editing except for physiologically impossible results.17
In conclusion we have shown the feasibility of a brachial cuff based method which allows combined ambulatory measurements of both brachial- and central BP and PWV for evaluation of the diurnal profile. PWV in type 2 diabetes was significantly lower during the night than in the day time and the within subject variation of heart rate, systolic aorta blood pressure and day/night status contributed independently to the variation of PWV. This brachial cuff based method demonstrates the same relation between AIXao, PWV and heart rate as known from invasive measurements of AIXao and studies using direct measurement of PWV.
The era of ambulatory measurement of PWV and central aortic BP has just begun. Comparing healthy subjects with different high risk populations including diabetes has a high priority in order to describe pathophysiological differences. Also the relation between changes in end organ damage (e.g. left ventricular mass) and changes in ambulatory central BP induced by pharmacological intervention is important.34 Prospective studies should reveal if these data are closer related to cardiovascular outcome data than ambulatory measurement of brachial BP or office PWV measurements.
Sources of funding
We have received a grant from
Conflicts of interest
None.
References
Cite this article
TY - JOUR AU - C. Krogager AU - N.B. Rossen AU - E. Laugesen AU - S.T. Knudsen AU - P.L. Poulsen AU - K.W. Hansen PY - 2014 DA - 2014/06/07 TI - 24-h ambulatory pulse wave velocity and central blood pressure in type 2 diabetes JO - Artery Research SP - 73 EP - 79 VL - 8 IS - 3 SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2014.04.004 DO - 10.1016/j.artres.2014.04.004 ID - Krogager2014 ER -