
Acute effect of coffee consumption on arterial stiffness, evaluated using an oscillometric method
- DOI
- 10.1016/j.artres.2017.01.001How to use a DOI?
- Keywords
- Vascular stiffness; Aorta; Caffeine; Blood pressure
- Abstract
Introduction: Previous studies show contradictory results related to the vascular effects of coffee; they suggest that caffeine increases arterial stiffness and negatively impacts vascular health, the aim of this study is to evaluate the acute coffee effects on the vascular stiffness.
Methods and materials: We carried out a controlled, blind, cohort study in healthy subjects. The acute effect of coffee (caffeinated vs. decaffeinated) was evaluated on arterial stiffness parameters, using a oscillometric method known as Arteriograph® (TensioMed-Budapest-Hungary, Ltd.). Each subject received 14 gr. of caffeinated excelso-coffee (caffeine-151.2 mg) and decaffeinated excelso-coffee (caffeine-3.92 mg), two weeks apart in a random order. The parameters were obtained under stable baseline conditions before drinking the coffee, 30 and 60 min later.
Results: Thirty-two subjects were included, with an age of 46.2 ± 10.4 years, sixteen men. Consumption of caffeinated-coffee at 30 and 60 min increased statistically significant (p < 0.05) brachial-systolic-blood-pressure in 3.9 mmHg and 3.8 mmHg, brachial-diastolic-blood-pressure in 4.1 mmHg and 3.2 mmHg, mean-arterial-pressure in 4.0 mmHg and 3.3 mmHg, central-systolic-blood-pressure in 5.8 mmHg and 7.6 mmHg, brachial-AIX 9.9% and 12.3%, aortic-AIX 5.1% and 6.3%, decreased heart-rate by 4 beats/min and 5 beats/min respectively, and it not demonstrated that had an impact on the pulse wave velocity (p = 0.861). Decaffeinated-coffee increased the braquial-AIX (7.1–10.5%) and aortic-AIX (3.55–5.3%) and decreased the heart-rate (3–4 beats/min).
Conclusions: This study suggests for the first time that drinking caffeinated coffee slightly increases peripheral arterial stiffness at the expense of increased vascular tone in distal arteries without changes in central stiffness. Further studies are needed to clarify whether these effects induced by coffee have an impact on the population health.
- Copyright
- © 2017 Association for Research into Arterial Structure and Physiology. Published by Elsevier B.V. All rights reserved.
- Open Access
- This is an open access article distributed under the CC BY-NC license.
Introduction
Cardiovascular disease continues to be the main cause of morbidity and mortality in the Western world.1 It is well known that a healthy and appropriate diet is the defining key for adequate human health, and the fundamental pillar for the prevention and treatment of cardiovascular diseases. Epidemiological and experimental studies in the last 50 years have implicated dietary factors in the etiology and prevention of important chronic diseases such as arteriosclerosis.2
Coffee is one of the most consumed beverages in the world. Among coffee’s components, the most recognized is caffeine, the active substance in many foods and beverages consumed around the world.3 Previous clinical studies have generated a significant controversy regarding the consumption of coffee and its cardiovascular effects.4–7 The divergence in clinical results is due to a high number of selection biases, and the presence o not of multiple risk factors which interact in the development of cardiovascular disease in humans. The results of controlled clinical studies in large populations have recently shown the benefits of coffee for cardiovascular health.7–9
Recently, the Scientific Report of the 2015 Dietary Guidelines Advisory Committee (DGAC), as the official organ of the Food and Drug Administration in the United States,10 described that the consumption of coffee within a moderate range (3–5 cups/day, or up to 400 mg/day of caffeine), is not associated with a greater risk of chronic diseases, such as cardiovascular disease, cancer and premature death in healthy adults. Consistent observation tests show that the moderate consumption of coffee is associated with a reduction in the risk of type II diabetes and cardiovascular disease, in healthy adults.11 Thus, the moderate consumption of coffee could be incorporated into a healthy lifestyle. The evidence suggests a significant inverse relationship between the consumption of 1–4 cups of coffee/day and total mortality, especially mortality due to cardiovascular disease.12–14 Previous studies by our group regarding the role of caffeine and its effect on in vitro animal15 and human16–18 arterial tissues, show beneficial vascular effects.
The study of vascular stiffness has generated great interest in the last two decades, especially the measurement of pulse wave velocity (PWV), measured in meters/sec, and the arterial augmentation indices, both brachial and aortic. The stiffening of the central arteries has important hemodynamic consequences which include: an increase in pulse pressure amplitude, decreased shear stress, and an increase in the transmission of the pulsatile flow within the microcirculation.19 These effects have adverse consequences, and could, in part, explain why arterial stiffness is a determinant of the cardiovascular system performance and a predictor of cardiovascular risk.20,21
Thus, arterial stiffness has been identified for several years as an independent cardiovascular risk factor.22–24 A high PWV has been shown to be associated with an increased risk of coronary disease, cerebrovascular accidents, and compound cardiovascular events.25,26
The vascular response in the presence of caffeine has been controversial. An acute vasopressor effect of caffeine has been described, mainly in non-habitual consumers. Current evidence supports the hypothesis that caffeine affects the cardiovascular system, at least acutely, not just through an elevation in peripheral blood pressure, but also through an increase in arterial stiffness.27
The current study intends to evaluate and quantify the in vivo effect of coffee on vascular mechanics, evaluated through vascular stiffness parameters using a non-invasive method, the Arteriograph® (TensioMed Budapest-Hungary, Ltd.), an available technology which uses an oscillometric method to detect brachial wave signals to evaluate vascular stiffness parameters, in a selected healthy population.
Materials and methods
This study was carried out in the Vascular Function Research Laboratory at the Fundación Cardioinfantil-Instituto de Cardiología, in Bogotá, Colombia. A controlled, blind, prospective cohort study was performed to evaluate the vascular effect of coffee, through measurement of vascular stiffness parameters in healthy adult individuals of both sexes, they were the self-controls using decaffeinated coffee. It was approved by the institutional Clinical Research and Research Ethics committees.
Inclusion criteria
Healthy individuals over the age of 30 and under the age of 60, who signed the informed consent.
Exclusion criteria
Cardiovascular disease conditions, such as heart failure, ischemic cardiopathy, arterial hypertension, renal insufficiency, diabetes mellitus. Conditions in which coffee consumption is contraindicated, such as: migraine, hyperthyroidism, cardiac tachyarrhythmias, anxiety states, symptomatic acute gastritis, diarrhea, and fibrocystic breast disease. Consumption of caffeinated beverages within the previous 12 h, alcohol, beta blockers, calcium channel blockers or nitrates, drug addiction, stimulant drugs (e.g. amphetamines), smoking, Raynaud’s phenomenon, vascular disease in upper limbs (e.g. AV fistula, brachial plexus compression syndrome) and high cardiac output diseases (anemia, thyrotoxicosis, fever, AV fistulas, aortic insufficiency).
Coffee and equipment used
The coffee was certified and supplied by the Federación Nacional de Cafeteros (FNC) de Colombia [Colombian National Federation of Coffee Growers]. This coffee was selected from the same lot, excelso type, Arabic variety. Part of this coffee underwent decaffeination techniques, removing approximately 97% of the caffeine content, and then had its physical and chemical properties analyzed in the Laboratorio de Análisis de Alma Café Descafecol [Alma Café Descafecol Analysis Laboratory]. Finally, the amount of caffeine was quantified in each of the coffees supplied; the caffeinated coffee has 1.23%, and the decaffeinated 0.03%. The physical and chemical properties are described in Table 1.
| Content | Roasted excelso coffee beans | Ground roasted excelso coffee | Decaffeinated ground roasted excelso coffee |
|---|---|---|---|
| Caffeine (% d.b.) | 1.19 | 1.23 | 0.03 |
| Moisture (%) | 3.24 | 4.32 | 3.78 |
| Fat content (%) | 24.269 | 14.373 | 14.368 |
| Chlorogenic acids (% d.b.) | |||
| 3-CQA | 0.5 | 0.36 | 0.35 |
| 5-CQA | 1.01 | 0.78 | 0.77 |
| 4-CQA | 0.61 | 0.46 | 0.46 |
| 3-FQA | 0.05 | 0.05 | 0.05 |
| 4-FQA | 0.02 | 0.02 | 0.02 |
| 5-CQA | 0.12 | 0.11 | 0.11 |
| 3,4 di-CQA | 0.03 | 0.02 | 0.02 |
| 3,5 di-CQA | 0.04 | 0.04 | 0.04 |
| 4,5 di-CQA | 0.04 | 0.02 | 0.03 |
| Sum CQA | 2.12 | 1.59 | 1.58 |
| Sum FQA | 0.19 | 0.18 | 0.18 |
| Sum di-CQA | 0.11 | 0.08 | 0.09 |
| Sum total CGA | 2.42 | 1.85 | 1.85 |
% d.b: Percentage, dry base, CQA: Caffeoylquinic acids, FQA: Feruloylquinic acids, CGA: Chlorogenic acids.
Coffee content.
The espresso coffee beverage was prepared in the Laboratory, always using the same routine technique, using a La Marzococco machine (ref: Alma Café 30002132). The coffee beans were ground using a La Cimbali machine (ref: Alma Café 30000046), with a grain size of 250 μm. For each patient, 14 gr. of ground coffee were used, producing a double espresso of approximately 65 ml. This volume of the coffee beverage contains 151.2 mg of caffeine and 3.92 mg, respectively. The Arteriograpgh® (TensioMed Budapest-Hungary, Ltd., Version 3.0.0.4) equipment uses oscillometric methods to achieve the complete evaluation of central and peripheral arterial function, which has been previously validated and described elsewhere.28,29
Validation of hemodinamic measurements
In order to validate the method of measuring non-invasive hemodynamic variables obtained with the oscillometric technique (equipment Arteriograph®, TensioMed, Budapest, Hungary, Ltd.), we conducted a simultaneous measurement using the left cardiac catheterization by radial technique (invasive hemodynamic) on a population of 100 consecutive adult patients. This prospective cohort observation was also approved by the Committees of Clinical Research and Ethics of the Institution.
The results show that the non-invasive method used in our study has a very good agreement with respect to the gold standard (cardiac catheterization). The intraclass correlation coefficient was greater than 0.9 in all variables, getting the same results using the Bland–Altman method (Table 2).30
| Variable | Non-invasive | Invasive | Δ | ICC | Min–Max |
|---|---|---|---|---|---|
| SBP-B (mmHg) | 140.7 ± 22.4 | 146.4 ± 22.8 | 5.7 ± 9.2 | 0.96 | 100–215 |
| DBP-B (mmHg) | 79.5 ± 12.1 | 74.6 ± 11.1 | −5.0 ± 7.5 | 0.90 | 46–109 |
| MAP-B (mmHg) | 100.3 ± 14.0 | 100.9 ± 13.4 | 0.6 ± 6.4 | 0.94 | 73–140 |
| HR (beats/min) | 71.3 ± 13.5 | 72.4 ± 13.4 | 1.1 ± 4.0 | 0.99 | 42–103 |
| SBP-Ao (mmHg) | 138.9 ± 26.7 | 139.6 ± 25.7 | 0.7 ± 6.1 | 0.99 | 94–217 |
| DBP-Ao (mmHg) | 79.9 ± 12.3 | 78.4 ± 11.4 | −1.5 ± 7.6 | 0.90 | 44–116 |
| MAP-Ao (mmHg) | 99.5 ± 15.5 | 102.5 ± 14.1 | 2.9 ± 6.6 | 0.96 | 73–148 |
Results expressed as mean ± standard deviation, Δ: difference between the two methods, ICC: Intraclass Correlation Coefficient, Min: minimum value of the sample, Max: maximum value of the sample. B: represents brachial or peripheral measurements. Ao: represents aortic or central measurements. SBP: Systolic blood pressure, DBP: Diastolic blood pressure, MAP: Medial blood pressure, HR: Heart rate.
Comparison results of the oscillometric non-invasive method versus the gold standard (invasive cardiac-catheterization).
Procedure
Once the fulfillment of inclusion and exclusion criteria had been verified, the study was verbally explained to the subjects, after which they signed the informed consent, and the following procedure was carried out. Thirty-two subjects underwent the test, first under baseline conditions, and then with caffeinated or decaffeinated coffee, randomly assigned, separated by a 15 ± 5.3 day interval.
Method for non-invasive hemodynamic measurements
All the selected individuals were given appointments in the morning, in a fasting state. Weight (kg) and height (cm) were recorded, and the data collection form (DCF) was completed for each of the subjects. Then, systolic (mmHg), diastolic (mmHg) and mean (mmHg) arterial pressure were measured, along with heart rate (beats/min) and vascular stiffness parameters, using the Arteriograph® (TensioMed Budapest-Hungría, Ltd.) system, after 15 min of rest on a cot in comfortable environmental conditions regarding temperature, light, humidity and noise. Then, each individal drank a dose of coffee (a double espresso of caffeinated or decaffeinated coffee, according to the study phase). All subjects underwent repeated measurements under the same conditions at 30 and 60 min after drinking the coffee, assuming that the maximum plasmatic concentration is obtained (Tmax) at 30–45 min, also there are no differences between 60 and 90 min and the maximum effecto of caffeine is around 60 min.10,18
Definition of variables
Habitual coffee drinkers were considered to be those subjects who drank at least one cup of coffee a day for the last week. Brachial systolic blood pressure (SBP-B, mmHg), brachial diastolic blood pressure (DBP-B, mmHg), mean arterial pressure (MAP, mmHg), brachial pulse pressure (PP-B, mmHg), HR: heart rate (beats/min), Brachial AIX: brachial augmentation index (%), Aortic AIX: central augmentation index (%), aortic pulse wave velocity (PWV, m/sec) is the pulse wave velocity in the aorta from the suprasternal notch to the pubis. Central systolic blood pressure (SBP-Ao, mmHg), aortic diastolic blood pressure (DBP-Ao, mmHg), central pulse pressure (PP-Ao, mmHg). The AIX measured by the device is corrected to a fixed HR (AIX@75).
Data collection form
A data collection form (DCF) was designed which included general demographic information, personal and family disease history, medications being taken at the time of data collection, usual consumption of coffee in the last month, physical activity and a report of the general physical exam. The complete data collection and DCF files were stored in a data base by one of the researchers, as they were obtained, and these were reviewed and validated jointly.
Good laboratory practice
This study was performed according to Good Clinical Practice. All patients were given a written description of the vascular stiffness study. All the data obtained remained in the local research center, in an Excel 2010 data base. The data were collected, analyzed and filed appropriately.
Sample size and statistical analysis
With sufficient power to detect significant differences in the values generated by the vascular effect of the consumption of coffee among individuals of both sexes, over the age of 30, assuming an alpha level of significance of 0.05, and an expected magnitude of the correlation coefficient of 0.25 (25% variation), a value determined by the researchers, and lacking studies that would provide similar values, a sample size was calculated of a minimum of 30 individuals in each group, from whom measurements were taken at baseline and after coffee consumption.
The statistical analysis was performed using the SPSS version 23 software belonging to the Fundación CardioInfantil-Instituto de Cardiología. Data are presented as mean ± standard deviation when the results are normally distributed, and as median (interquartile range) when they are not. The normality of the samples was evaluated using the Shapiro–Wilk test. The Student t test was used to determine the significance of normally distributed parametric values, and the Wilcoxon rank test for those not normally distributed. A p value less than 0.05 is considered statistically significant.
The changes in arterial stiffness parameters were analyzed at three points in time (baseline, 30 min and 60 min). First of all, the baseline measurements of both moments were evaluated, evaluating the reproducibility of the technique employed, then the changes after consuming caffeinated coffee, decaffeinated coffee, and the changes between the two coffees. The first two were performed with tests for a related sample, and the last where changes are compared using a t test for independent samples, or a non-parametric Mann–Whitney U test, taking into account the difference between the coffees. Also the results were analyzed by repeated-measures ANOVA. The total results are represented in tables and the most significant results in various graphics.
Results
Thirty-two healthy subjects were included in the study, with an average age of 46.2 ± 10.4 years. Sixteen males with an age of 53.518 years, of which 14 (87.5%) were habitual coffee drinkers. Sixteen women with an age of 43.021 years (p = NS), of which 14 (87.5%) (p = NS) were habitual coffee drinkers (Tables 3–4).
| Variable | n (32) |
|---|---|
| Age (years) | 46.2 ± 10.4 |
| Sex. Males(n) | 16 (50%) |
| Weight (Kg) | 67.3 ± 10.5 |
| Height (cm) | 166.3 ± 9.5 |
| Body mass index | 24.3 ± 2.8 |
| Habitual coffee consumers | 28 (87.5%) |
| Frequency of coffee consumption | |
| 1–2 Cups/Week | 15 |
| 3–4 Cups/Week | 7 |
| 5–6 Cups/Week | 4 |
| >6 Cups/Week | 2 |
Results expressed as mean ± standard deviation.
Demographic results.
| Variable | Males. n (16) | Females. n (16) | p value |
|---|---|---|---|
| Age (years)a | 53.5 (18) | 43.0 (21) | 0.186 |
| Weight (Kg)b | 73.5 ± 9.4 | 61.13 ± 7.5 | <0.001 |
| Height (cm)a | 173.5 (8.75) | 157.5 (5) | <0.001 |
| Body mass indexb | 24.36 ± 2.4 | 24.20 ± 3.2 | 0.877 |
| Habitual coffee consumer (n-%) | 14 (87.5%) | 14 (87.5%) | 1 |
Bold means statistical significance p value.
Results expressed as median and interquartile range.
Results expressed as mean ± standard deviation.
Results by sex.
Results under baseline conditions prior to caffeinated coffee consumption
The results of measurements under baseline conditions prior to consuming caffeinated and decaffeinated coffee are shown in Table 5. They show how the hemodynamic conditions are very similar, except for the heart rate, which increased by three beats (p = SS), and the Brachial AIX and Aortic AIX which were slightly more negative at the control time (p = SS).
| Variable | Initial baseline | Control baseline | p value |
|---|---|---|---|
| SBP-B (mmHg)b | 118.28 ± 10.6 | 116.9 ± 8.3 | 0.338 |
| DBP-B (mmHg)b | 74.59 ± 8.5 | 72.7 ± 8.8 | 0.214 |
| PP-B (mmHg)a | 43.5 (8.0) | 43.5 (7.0) | 0.905 |
| MAP (mmHg)b | 89.22 ± 9 | 87.5 ± 8.3 | 0.188 |
| HR (beats/min)b | 56.88 ± 9.6 | 59.1 ± 9.9 | 0.038 |
| Brachial AIX (%)a | −11.9 (49.1) | −25.0 (52.5) | 0.012 |
| SBP-Ao (mmHg)a | 113.9 (13.1) | 111.5 (21.1) | 0.100 |
| DBP-Ao (mmHg)b | 74.61 ± 8.5 | 72.9 ± 8.8 | 0.213 |
| PP-Ao (mmHg)a | 41.6 (10.6) | 39.6 (10.3) | 0.179 |
| Aortic AIX (%)a | 31.6 (24.8) | 25.0 (26.5) | 0.012 |
| PWV (m/s)a | 7.10 (1.4) | 6.95 (1.65) | 0.940 |
Bold means statistical significance p value.
Results expressed as median and interquartile range.
Results expressed as mean ± standard deviation. B: represents brachial or peripheral measurements. Ao: represents aortic or central measurements. SBP: Systolic blood pressure, DBP: Diastolic blood pressure, PP: Pulse pressure, MAP: Medial blood pressure, HR: Heart rate, AIX: augmentation index, PWV: Pulse wave velocity.
Comparison results of subjects under baseline conditions at the two evaluation times.
Comparison of baseline conditions versus at 30 and 60 min after drinking caffeinated coffee
The results of Table 6 shows how the intake of caffeinated coffee increases SBP-B, DBP-B, and MAP, slightly reduces the HR, increases SBP-Ao, DBP-Ao, brachial AIX and aortic AIX, without significant changes being detected in PWV. It is important to highlight that Brachial AIX changes from negative to positive. These effects are sustained at 30 and 60 min (Figs. 1–10, Panel A).
| Variable | Baseline | 30′ | Δ | p value | 60′ | Δ | p value |
|---|---|---|---|---|---|---|---|
| SBP-B (mmHg)b | 118.28 ± 10.6 | 122.16 ± 10.8 | 3.88 | 0.040 | 122.09 ± 11.8 | 3.81 | 0.005 |
| DBP-B (mmHg)b | 74.59 ± 8.5 | 78.69 ± 7.9 | 4.09 | 0.004 | 77.75 ± 9.3 | 3.16 | 0.009 |
| PP-B (mmHg)a | 43.5 (8.0) | 41.5 (8.3) | −2.00 | 0.488 | 44.0 (8.3) | 0.50 | 0.488 |
| MAP (mmHg)b | 89.22 ± 9.0 | 93.22 ± 8.5 | 4.00 | 0.005 | 92.53 ± 9.9 | 3.31 | 0.004 |
| HR (beats/min)b | 56.88 ± 9.6 | 53.69 ± 8.4 | −3.19 | 0.001 | 51.94 ± 7.8 | −4.94 | <0.001 |
| Brachial AIX (%)a | −11.90 (49.1) | 7.95 (52.73) | 19.85 | <0.001 | 8.10 (55.1) | 20.00 | <0.001 |
| SBP-Ao (mmHg)a | 113.90 (13.1) | 119.65 (15.2) | 5.75 | <0.001 | 121.50 (20.9) | 7.60 | <0.001 |
| DBP-Ao (mmHg)b | 74.61 ± 8.5 | 78.68 ± 7.9 | 4.08 | 0.002 | 77.76 ± 9.3 | 3.16 | 0.003 |
| PP-Ao (mmHg)a | 41.65 (10.6) | 43.50 (8.8) | 1.85 | 0.026 | 44.00 (8.7) | 2.35 | 0.026 |
| Aortic AIX (%)a | 31.60 (24.8) | 41.65 (26.7) | 10.05 | <0.001 | 41.75 (27.9) | 10.15 | <0.001 |
| PWV (m/s)a | 7.10 (1.4) | 7.00 (1.1) | −0.10 | 0.648 | 7.10 (0.9) | 0.00 | 0.648 |
Bold means statistical significance p value.
Results expressed as median and interquartile range.
Results expressed as mean ± standard deviation. B: represents brachial or peripheral measurements. Ao: represents aortic or central measurements. SBP: Systolic blood pressure, DBP: Diastolic blood pressure, PP: Pulse pressure, MAP: Medial blood pressure, HR: Heart rate, AIX: augmentation index, PWV: Pulse wave velocity.
Comparison results of subjects under baseline conditions compared with the consumption of caffeinated coffee at 30 and 60 min.

Behavior of heart rate in the presence of caffeinated coffee (A), decaffeinated coffee (B), and a comparison between the two groups (C). *p < 0.005 **p < 0.001.
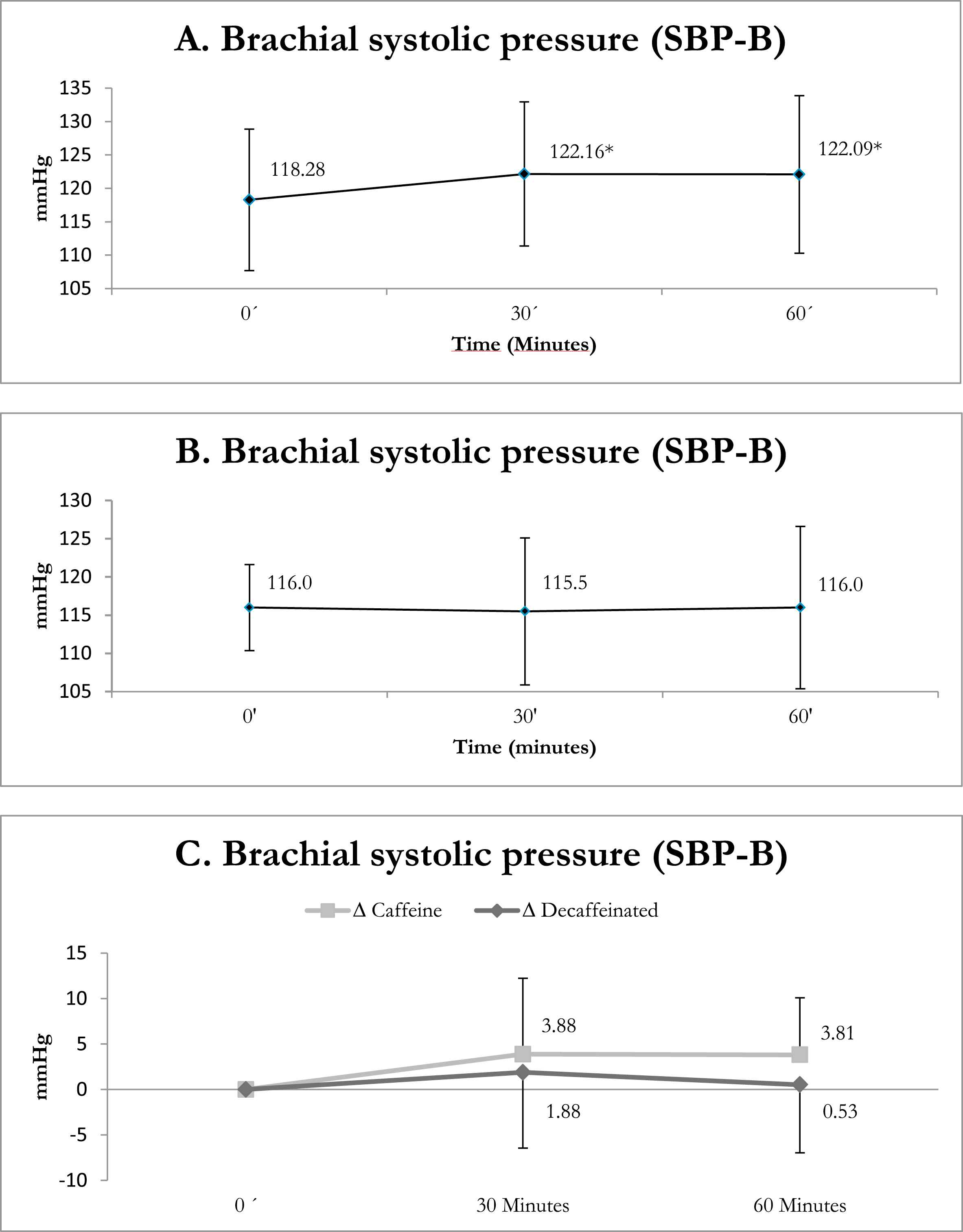
Behavior of brachial systolic blood pressure in the presence of caffeinated coffee (A), decaffeinated coffee (B), and a comparison between both groups (C). *p < 0.005 **p < 0.001.

Behavior of brachial diastolic blood pressure in the presence of caffeinated coffee (A), decaffeinated coffee (B), and a comparison between both groups (C). *p < 0.005 **p < 0.001.
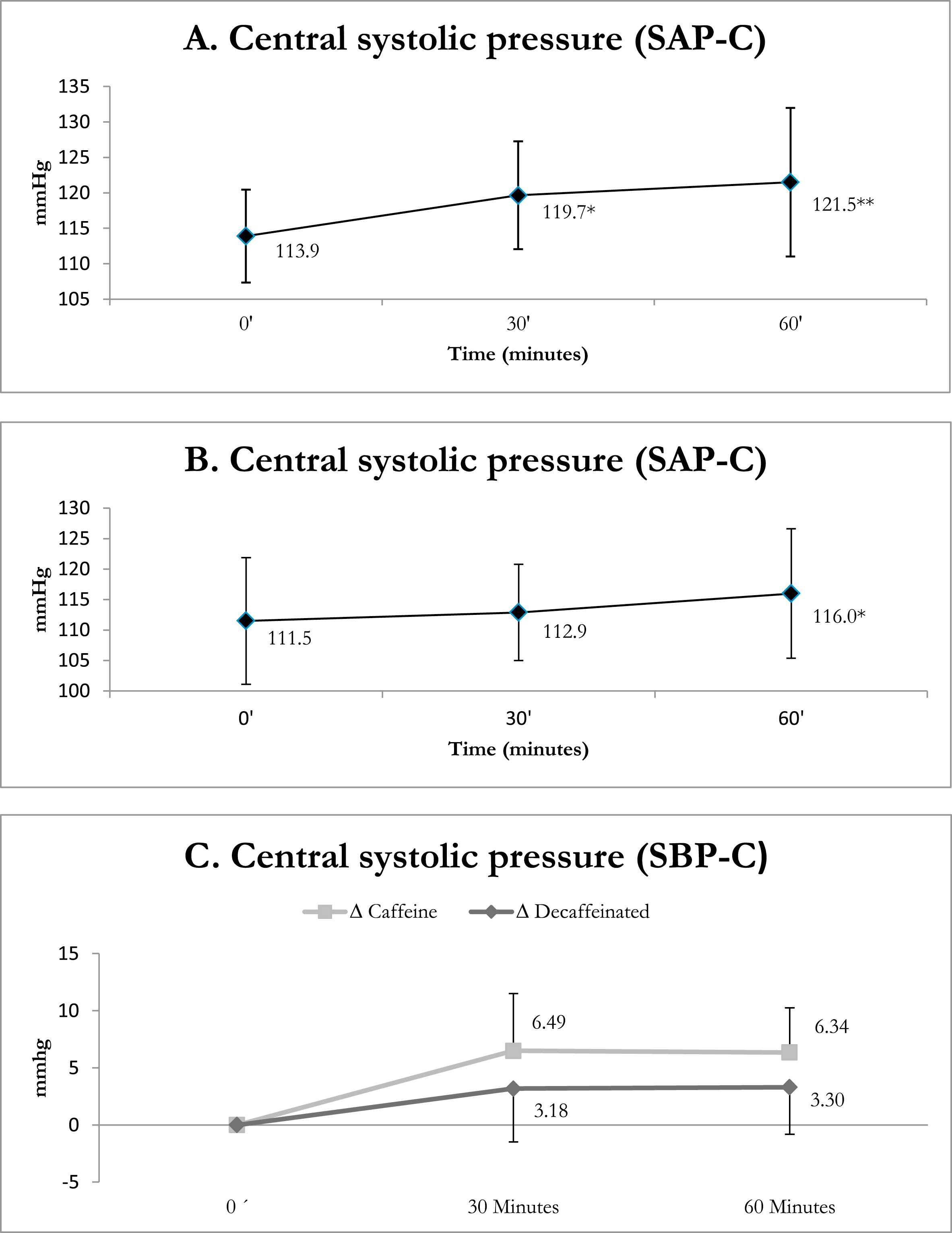
Behavior of central systolic blood pressure in the presence of caffeinated coffee (A), decaffeinated coffee (B), and a comparison between the two groups (C). *p < 0.005 **p < 0.001.

Behavior of central diastolic blood pressure in the presence of caffeinated coffee (A), decaffeinated coffee (B), and a comparison between both groups (C). *p < 0.005 **p < 0.001.

Behavior of brachial pulse pressure in the presence of caffeinated coffee (A), decaffeinated coffee (B) and a comparison between the two groups (C). *p < 0.005 **p < 0.001.

Behavior of central pulse pressure in the presence of caffeinated coffee (A), decaffeinated coffee (B) and a comparison between both groups (C). *p < 0.005 **p < 0.001.
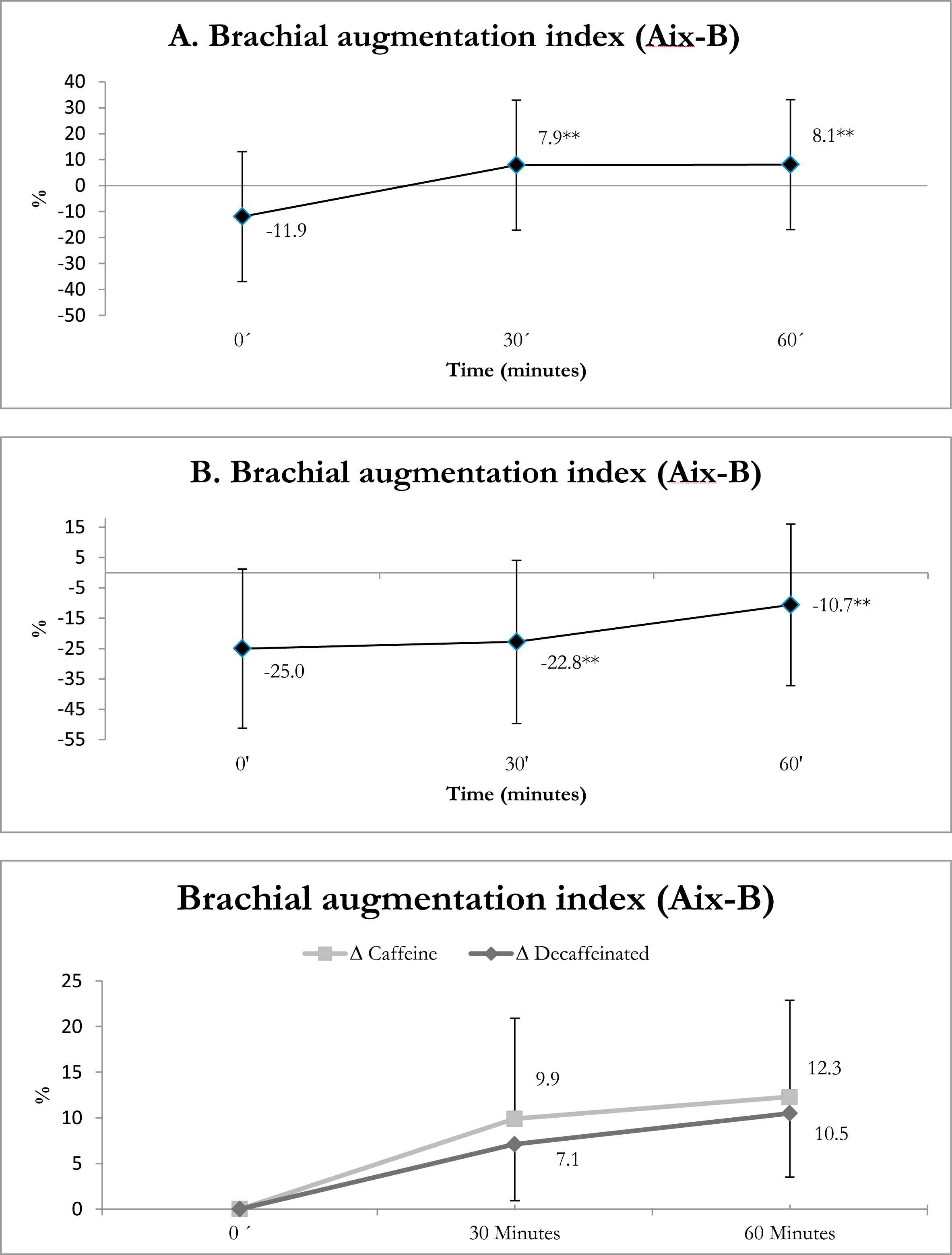
Behavior of the brachial augmentation index in the presence of caffeinated coffee (A), decaffeinated coffee (B), and a comparison between both groups (C). *p < 0.005 **p < 0.001.

Behavior of the central augmentation index in the presence of caffeinated coffee (A), decaffeinated coffee (B), and a comparison between the two groups (C). *p < 0.005 **p < 0.001.
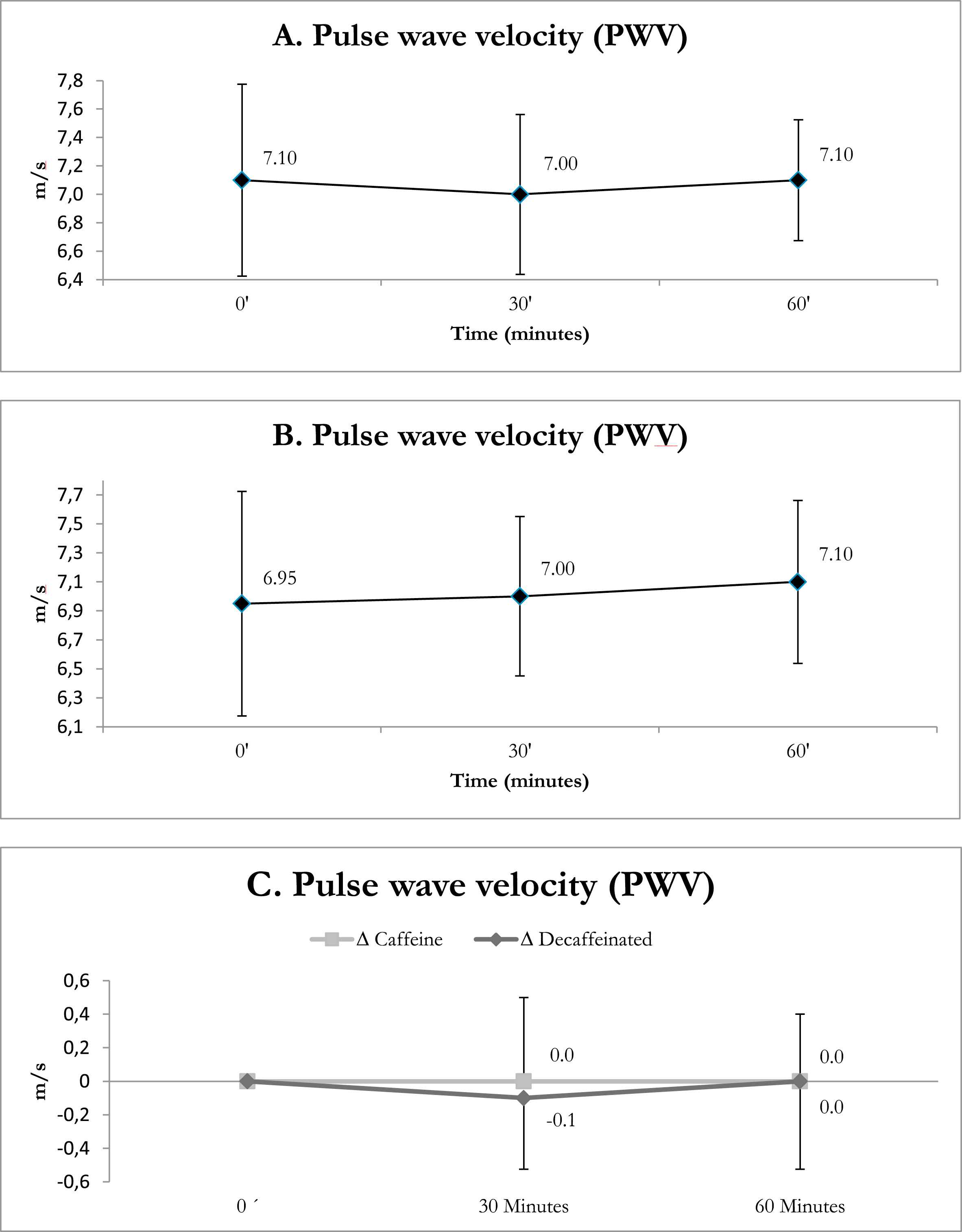
Behavior of pulse wave velocity in the presence of caffeinated coffee (A), decaffeinated coffee (B), and a comparison between both groups (C). *p < 0.005 **p < 0.001.
Comparison of baseline conditions versus those at 30 and 60 min after drinking decaffeinated coffee
Table 7 shows how the intake of decaffeinated coffee has a slight impact on brachial and aortic PP, reduces the heart rate, and increases the AIXes (p = SS) notably less than the effect of caffeinated coffee. These effects are also sustained at 30 and 60 min. No significant changes in PWV were detected, either (Figs. 1–10, Panel B).
| Variable | Baseline | 30′ | Δ | p value | 60′ | Δ | p value |
|---|---|---|---|---|---|---|---|
| SBP-B (mmHg)a | 116.0 (11.9) | 115.5 (19.7) | −0.50 | 0.345 | 116.0 (21.8) | 0.00 | 0.345 |
| DBP-B (mmHg)b | 73.0 ± 8.8 | 72.9 ± 9.6 | 0.0 | >0.999 | 74.8 ± 8.3 | 1.8 | 0.179 |
| PP-B (mmHg)a | 43.5 (7.0) | 44.5 (10.5) | 1.00 | 0.008 | 41.0 (6.8) | −2.50 | 0.008 |
| MAP (mmHg)b | 87.5 ± 8.3 | 88.3 ± 10.0 | 0.7 | >0.999 | 89.0 ± 9.3 | 1.5 | 0.302 |
| HR (beats/min)b | 59.1 ± 9.9 | 56.1 ± 8.5 | −3 | 0.001 | 55.0 ± 7.8 | −4.1 | <0.001 |
| Brachial AIX (%)a | −25.0 (52.5) | −22.8 (53.8) | 2.15 | <0.001 | −10.7 (53.3) | 14.30 | <0.001 |
| SBP-Ao (mmHg)a | 111.5 (21.1) | 112.9 (20.6) | 1.40 | 0.223 | 111.3 (27.8) | −0.20 | 0.223 |
| DBP-Ao (mmHg)b | 73.0 ± 8.8 | 72.9 ± 9.6 | 0.0 | >0.999 | 74.8 ± 8.3 | 1.8 | 0.181 |
| PP-Ao (mmHg)a | 39.6 (10.3) | 40.9 (12.1) | 1.35 | 0.021 | 39.3 (15.0) | −0.25 | 0.021 |
| Aortic AIX (%)a | 25.0 (26.5) | 26.1 (27.2) | 1.10 | <0.001 | 32.3 (27.0) | 7.25 | <0.001 |
| PWV (m/s)a | 6.95 (1.65) | 7.00 (1.1) | 0.05 | 0.374 | 7.10 (1.2) | 0.15 | 0.374 |
Bold means statistical significance p value.
Results expressed as median and interquartile range.
Results expressed as mean ± standard deviation. B: represents brachial or peripheral measurements. Ao: represents aortic or central measurements. SBP: Systolic blood pressure, DBP: Diastolic blood pressure, PP: Pulse pressure, MAP: Medial blood pressure, HR: Heart rate, AIX: augmentation index, PWV: Pulse wave velocity.
Comparison results of subjects under baseline conditions compared with the consumption of decaffeinated coffee at 30 and 60 min.
Comparison of changes with the intake of caffeinated and decaffeinated coffee at 30 and 60 min
Table 8 shows how the intake of coffee presents some changes independently of the presence or absence of caffeine. There are significant changes in DBP-B and DBP-C. An increase in the AIXes can be seen, but the more drastic effect of caffeinated coffee must be taken into account; the value changes from negative to positive. Significant changes in PWV were not seen, either (Figs. 1–10, Panel C).
| Variable | 30 min | 60 min | ||||
|---|---|---|---|---|---|---|
| Δ Caffeine |
Δ Decaffeinated |
p value | Δ Caffeine |
Δ Decaffeinated |
p value | |
| SBP-B (mmHg)b | 3.88 ± 8.3 | 1.88 ± 8.3 | 0.341 | 3.81 ± 6.3 | 0.53 ± 7.5 | 0.062 |
| DBP-B (mmHg)b | 4.09 ± 6.6 | −0.03 ± 6.2 | 0.012 | 3.16 ± 5.6 | 1.81 ± 5.3 | 0.324 |
| PP-B (mmHg)b | −0.22 ± 6.6 | 1.91 ± 5.1 | 0.152 | 0.66 ± 5.4 | −1.28 ± 7.1 | 0.097 |
| MAP (mmHg)b | 4.00 ± 6.6 | 0.72 ± 6.6 | 0.051 | 3.31 ± 5.3 | 1.50 ± 5.0 | 0.163 |
| HR (beats/min)a | −4.00 (4.3) | −3.00 (5.3) | 0.936 | −5.00 (5.3) | −4.00 (5.5) | 0.475 |
| Brachial AIX (%)a | 9.90 (22.0) | 7.10 (12.4) | 0.219 | 12.25 (21.2) | 10.5 (14.0) | 0.656 |
| SBP-Ao (mmHg)b | 6.49 ± 10.0 | 3.18 ± 9.3 | 0.176 | 6.34 ± 7.8 | 3.30 ± 8.2 | 0.135 |
| DBP-Ao (mmHg)b | 4.08 ± 6.6 | −0.03 ± 6.2 | 0.013 | 3.16 ± 5.6 | 1.81 ± 5.3 | 0.327 |
| PP-Ao (mmHg)b | 2.42 ± 6.9 | 3.21 ± 5.6 | 0.614 | 3.18 ± 5.1 | 1.49 ± 6.5 | 0.254 |
| Aortic AIX (%)a | 5.05 (11.1) | 3.55 (6.3) | 0.209 | 6.25 (10.8) | 5.30 (7.1) | 0.646 |
| PWV (m/s)a | 0.00 (0.7) | −0.10 (0.9) | 0.105 | 0.00 (1.0) | 0.00 (1.0) | 0.877 |
Bold means statistical significance p value.
Results expressed as median and interquartile range.
Results expressed as mean ± standard deviation. B: represents brachial or peripheral measurements. Ao: represents aortic or central measurements. SBP: Systolic blood pressure, DBP: Diastolic blood pressure, PP: Pulse pressure, MAP: Medial blood pressure, HR: Heart rate, AIX: augmentation index, PWV: Pulse wave velocity.
Comparison results of the changes comparing the consumption of coffee with that of decaffeinated coffee at 30 and 60 min.
Discussion
In this blind controlled clinical study designed to evaluate the acute effects (30 and 60 min) of caffeinated and decaffeinated coffee consumption on arterial stiffness in a healthy adult population using the oscillometric method with Arteriograph® (TensioMed Budapest, Hungary, Ltd.) equipment, caffeinated coffee was shown to have a greater acute effect on arterial stiffness than decaffeinated coffee, considering the increase in SBP-B, SBP-Ao and a significant increase in the AIXes, in spite of not registering significant changes in the PWV. These findings suggest an acute effect of caffeine on peripheral arteries (muscular and arterioles), increasing arterial tone and reflecting an increased sustained arterial stiffness at 60 min. The lack of involvement of the PWV could probably be explained by an effect on the reduction of the heart rate, or a relative insensitivity of the aorta (elastic arteries) to coffee’s effect.
In our study, we tried to have homogenous populations as well as some characteristics that make it different from previous studies. The protocol was very strict in the selection of the type of coffee and its preparation, in an attempt to simulate the optimal conditions of a healthy person in his/her real life. As previously described, the coffee was certified and supplied by the FNC, selected from the same lot, excelso type, Arabic variety. Part of the same coffee underwent decaffeination techniques; the coffee espresso beverage was prepared in the Laboratory, always using the same routine technique. In addition, it was a healthy population of young adults, without risk factors for cardiovascular disease. The vast majority were habitual mild consumers of caffeine; however, they all entered measurements with more than 12 h of fasting.
Many observational epidemiological studies and clinical assays have shown a strong association between PP-B measured by sphygmomanometer and adverse cardiovascular events, including mortality.31–33 Given that PP-B is related to the physical properties of elastic arteries, much of the attention has been directed towards arterial stiffness, PWV, and wave reflection as independent cardiovascular risk factors. In fact, independent studies have shown that central arterial stiffness increases in older people,34–36 and in patients with coronary artery disease,37,38 myocardial infarction,39 heart failure,40 hypertension,23,41–44 cerebrovascular accidents,45 diabetes mellitus,46 end stage renal disease,47,48 and hypercholesterolemia.49 In addition, recent studies have shown that aortic pulse pressure is a better predictor of the thickness of the intima-media in the carotids,50 restenosis following coronary angioplasty,51 and severity of coronary artery disease.52 On the other hand, the beneficial reduction of SBP-Ao and PP-Ao with vasodilators drugs is underestimated by measurements of SBP-B.53–55 This disparity is due to the amplitude and time of the pressure waves reflected from the periphery.56–59 Important changes in central elastic arteries are produced over time, and acute alterations in the arterial wall properties are passive, while changes in muscular arteries and arterioles occur more often acutely, and the alterations in the wall properties are active.60 A change in the stiffness of muscular arteries is mainly due to the acute changes in tone of the arterial smooth muscle.
The PWV is widely recognized as a direct marker of arterial stiffness.61–64 The AIX is considered to be an indirect marker of arterial stiffness and a direct measure of wave reflection.55–65
Much accumulated evidence suggests that the consumption of caffeine induces an increase in SBP (predominantly) and a slight increase in DBP, mainly in chronic coffee consumers.66,67 During the last decade, researchers have begun by examining the acute effects of caffeine on arterial stiffness. The topic is disproportionately unexplored, compared to the wide use of this substance. Over the last two decades, there has been an interest in quantifying the effect of caffeine on vascular stiffness. Several previous studies have suggested that the consumption of caffeine increases arterial stiffness, and could have an adverse effect on vascular health. In 2001, a study with a limited number of healthy subjects stated, for the first time, that caffeine had adverse effects on arterial vascular stiffness.68 Vlachopoulos et al.,69 found for the first time that caffeine could increase wave reflection in hypertensive patients, and it was hypothesized that caffeine could increase arterial stiffness. In 2003, the same group published results of the effect of the consumption of 250 mg of caffeine on the elastic properties of the aorta and wave reflection, in 20 healthy subjects in a randomized, controlled study with placebo,70 using a Complior® (Dupont Medical, Pantin, France) tonometric method. The results were that PWV increases (0.51 m/sec; p < 0.001), which denotes an increase in aortic stiffness. The AIX and heightened pressure increased (6.8% and 4.4 mmHg, respectively; p < 0.001 for both) which denotes an increase in wave reflections. At the same time, SBP-B, SBP-Ao, DBP-B, DBP-Ao and PP-Ao all increased significantly, concluding that the consumption of caffeine is associated with an acute and unfavorable effect on the elastic properties of the aorta and wave reflection. In 2003,71 results were published of an observation of aortic stiffness measured by carotid-femoral PWV (Complior, Dupont Medical, Pantin, France) in 12 hypertensive patients exposed to 250 mg of caffeine (a dose equivalent to 2 to 3 cups of coffee), in which they found that SAP and PP increased significantly (12.3; p = 0.005 and 7.4 mmHg; p < 0.01, respectively), while DBP showed no changes. The PWV increased (0.57 m/sec, p < 0.05), denoting an increase in aortic stiffness with a peak at 60 min, and decreasing progressively over time, describing for the first time that caffeine has an acute unfavorable effect on arterial stiffness in hypertensive patients who are habitual consumers of caffeine.
In 2005, the same group72 once again described the results of the chronic consumption of coffee on the elastic properties of the aorta. They found a linear relationship between the consumption of coffee and PWV, AIX, and pressure increase. Compared with the non-coffee consuming group, the PWV increased 13%, the AIX doubled, and the arterial pressure was higher in the high coffee consumption group. These findings were statistically significant. In 2007, in a series of 259 hypertensive patients exposed to chronic coffee consumption,73 the post hoc analyses showed that all the coffee consumption groups had higher AIXes compared to non-consumers. PWV did not differ between the daily coffee consumption groups. Each participant had a 35% greater relative risk of having a high AIX, for each cup (150 mL) of coffee per day, and a 40% greater relative risk for every 10 cups/day. This is the first study to show that, in hypertensive patients, the consumption of coffee is associated with an increase in wave reflections, but is not associated with aortic stiffness. Curiously, the results of that study are not a direct extrapolation of the findings in normotensive subjects, since, unlike these, only wave reflections are affected, which indicates a different behavior of the large and small arteries in hypertension.
Finally, we have shown the effects of caffeinated and decaffeinated coffee consumption on the vascular stiffness. Assuming the AIX is better in young adults and PWV better in older adults,74,75 we have exposed that coffee with and without caffeine increases the AIX, the caffeinated increases it more than the decaffeinated coffee. It is important to know that the decaffeinated coffee has a small quantity of caffeine, but the other vasoactive components of coffee are also important on the vascular system.76 This could explain the effects on the peripheral arteries, something different shown by Mahmud and Feely using the tonometric method.68
Limitations
Among the possible limitation of the study is the lack of quantification of serum levels of caffeine in the patients. Given the results, the continuous and progressive administration of caffeinated coffee in increasing doses could have supplied complementary information regarding the effect of coffee on arterial stiffness, to see the dose–response ratio.
Conclusions
Unlike previously published studies using tonometric methods, in the present study, using the described technique (oscillometric method), we showed that the consumption of caffeinated coffee (two espressos with a concentration of 151.2 mg of caffeine, corresponding to two cups of coffee) slightly increases peripheral arterial stiffness due to an increase in vascular tone in distal arteries (muscular and arterioles), suggested by the increase in SBP and the AIXes, without changes in central stiffness. The current results help clarify even more the vascular effects of coffee consumption in the healthy population, but further studies are needed to clarify whether these effects induced by coffee have an impact on the population health.
Declaration of conflicts of interest
The authors express that they have no conflict of interest. This study was carried out with funds belonging to the Institution, as a research line of the Vascular Function Research Laboratory at the Fundación CardioInfantil-Instituto de Cardiología.
Acknowledgements
Dr. Daniel G. Acuña, Msc., of the Federación Nacional de Cafeteros de Colombia, for his constant consultancy. Luz D. Cárdenas for her help in carrying out the exams, and to Karen Moreno for the statistical analyses.
References
Cite this article
TY - JOUR AU - Darío Echeverri AU - Alejandro Pizano AU - Félix R. Montes AU - Pedro Forcada PY - 2017 DA - 2017/01/27 TI - Acute effect of coffee consumption on arterial stiffness, evaluated using an oscillometric method JO - Artery Research SP - 16 EP - 32 VL - 17 IS - C SN - 1876-4401 UR - https://doi.org/10.1016/j.artres.2017.01.001 DO - 10.1016/j.artres.2017.01.001 ID - Echeverri2017 ER -